Article Text

Abstract
Background The worldwide number of refugees has considerably increased due to ongoing wars, national instability, political persecution and food insecurity. In Europe, about one-third of all refugees are children, an increasing number of which are travelling alone. There are often no systematic medical health assessments for these refugee children on entry in reception countries despite the fact that they are recognised as an at-risk population due to increased burden of physical and mental health conditions. We aimed to perform a systematic review of the literature to describe the health status of refugee children on entering reception countries.
Methods A systematic search of published literature was conducted using the terms refugee, immigrant or migrant, medical or health, and screening.
Results Of the 3487 potentially relevant papers, 53 population-based studies were included in this review. This systematic review showed that refugee children exhibit high estimated prevalence rates for anaemia (14%), haemoglobinopathies (4%), chronic hepatitis B (3%), latent tuberculosis infection (11%) and vitamin D deficiency (45%) on entry in reception countries. Approximately one-third of refugee children had intestinal infection. Nutritional problems ranged from wasting and stunting to obesity.
Conclusions Refugee children entering reception countries should receive comprehensive health assessments based on the outcomes of this systematic review, national budgets, cost-effectiveness and personal factors of the refugees. The health assessment should be tailored to individual child health needs depending on preflight, flight and postarrival conditions.
A paradigm shift that places focus on child health and development will help this vulnerable group of children integrate into their new environments.
PROSPEROregistrationnumber
122561.
- tropical paediatrics
- paediatric practice
- infectious diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The global population of forcibly displaced persons has substantially increased over the last two decades (ie, from 37.3 million individuals in 1996 to 68.5 million in 2018).1 Throughout 2016, 1.2 million new refugees and asylum seekers (box 1) arrived in Europe, thus increasing the total number of refugees living within the continent to just under 4.4 million.2
Definitions
In this article, the term ‘refugee children’ is used to describe the entire child population of asylum seekers, refugees, status-holders and undocumented migrants. The term ‘children from refugee and refugee-like backgrounds’ is also widely used. There is no universally accepted term to describe refugee children.
Refugee: An asylum seeker that has fled their home country and has a ‘well-founded fear of persecution’ if they return home. Refugee status is granted when an asylum seeker has been acknowledged as a refugee according to the United Nations Refugee Convention. A refugee has completed the asylum process when they have been granted a residence permit.34
Asylum seeker: An individual who has left their home country and calls on the protection of another country and whose request for sanctuary has yet to be processed.35
Unaccompanied minor or unaccompanied minor refugee: An individual under the age of 18 applying for asylum without a relative older than 18 years of age. In the past, this group was also referred to as unaccompanied minor asylum seekers.
This global humanitarian situation is complicated by the fact that approximately half of all refugees and asylum seekers worldwide are children. Eurostat numbers indicate that nearly 400 000 children claimed asylum in Europe in 2016; 15.9% of these children were registered as unaccompanied minors.2 Country of origin, ethnicity and preflight conditions are all factors that contribute to the unique health risks of refugee children. Previous research has also shown that refugee children often have complex healthcare needs.3 The health status of many children residing in reception countries is known through antenatal screening, neonatal screening, immunisation programmes and regular medical follow-ups. However, this is often not the case for refugee children.
We aimed to systematically review the literature to describe the health status of refugee children on entering reception countries. Specifically to describe the prevalence of anaemia, haemoglobinopathies (HbP), infectious diseases, growth and nutrition disorders as identified through health screening programme and their vaccination status.
Health concerns in refugee children
Anaemia and genetic disorders of the red blood cells
Anaemia is a significant public health problem worldwide. A WHO global report revealed that children are prone to developing anaemia if they reside in a country with a high burden of infectious diseases, nutritional deficiencies or HbP. Among refugee children in Jordan in 2014, 48% of the children living in Zaatari refugee camp suffered from any kind of anaemia. Refugee children residing outside the camp were better off with 26% suffering from anaemia.4 For refugee children entering the USA, Yun et al found anaemia prevalence ranging from 6% to 23% depending on the country of origin, with the highest prevalence up to 35% in children less than 5 years of age.3 Similar results were found by Geltman et al among refugee children entering the Massachusetts between 1995 and 1998, with 12% of anaemia in the overall population and 28% in the group younger than 2 years.5 Anaemia increases the risk of child morbidity and mortality while also contributing to poor physical and cognitive development and performance.6 Disorders of the red blood cells, HbP (eg, sickle cell disease), thalassemia and glucose-6-phosphate dehydrogenase (G6PD) deficiency are common genetic conditions in children originating from Africa, Asia and the Middle East. These disorders not only contribute to the development of anaemia in carriers, but they can also lead to severe diseases, adverse birth outcomes and lowered life expectancy rates.7 Hereditary and metabolic disorders are also responsible for a substantial number of infant morbidities and mortalities in Arab countries. A total of 60% of children born to Iraqi refugees settling in the USA had parents from the same ethnic group or who were consanguine; this may account for their high prevalence of inherited blood disorders (ie, G6PD (39.5/10 000) and thalassemia (10.5/10 000)).8
Infectious diseases
Although the hepatitis B virus (HBV) disease can be prevented through vaccination, HBV infection remains a major public health problem globally. Perinatal infections with HBV in children result in chronic HBV infections in 90% of all cases; additionally, 25% of these affected children will develop primary liver cancer or cirrhosis as adults. The estimated global prevalence of the disease is 3%.9 However, there is wide regional variation in this number also seen in refugee children.9 10 Chronic hepatitis B infection was found in 4% of refugee children attending a specialist health clinic in Sydney and in 8% of the unaccompanied minor refugees in Germany.10 11The Joint UnitedNations Programme on HIV and AIDS estimate indicated that approximately 1.8 million children under the age of 15 were living with HIV. Prevalence data for HIV among refugee children are scarce because HIV testing is not routinely performed. Circumstantial evidence from the Netherlands were 80 out of 4854 pregnant asylum-seeking women were found to be living with HIV in the period from 2000 to 2008. Among African pregnant women, the prevalence rate was 3.4% compared with 0.04% in women from other regions. Women arriving without a partner and unaccompanied minors had higher HIV prevalence rates.12
Tuberculosis (TB) is one of the leading worldwide causes of death from infectious disease. The disease is steadily declining in most Western countries, but migration, poverty, war and political instability provide a perfect breeding ground for its resurgence.13 Twenty-five per cent of the refugee children entering Massachusetts between 1995 and 1998 had a positive skin test for latent TB and 21% of these children were found with intestinal parasites.5
Growth and nutrition
In 2014, little evidence was found for severe acute malnutrition in Syrian refugee children in a Jordan refugee camp.4 14 Growth abnormalities among recently arrived refugee children are common, showing both growth retardation and overweight and obesity.5
Vaccine coverage
Although vaccine uptake has increased on a worldwide scale as U5 mortality has decreased, there has been a resurgence of vaccine-preventable diseases such as measles, polio and diphtheria among refugee children in war zones and other unstable areas.11
Methods
Search strategy and eligibility criteria
This systematic review was performed and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.15 We conducted a systematic search for published articles related to the study intent in PubMed, EMBASE and the Web of Science database between 1 January 2007 and 1 April 2018. We developed a search strategy that was adapted for each database using a combination of medical subject headings, including terms related to refugee/migrant/immigrant, medical/health and screening. We supplemented this search by using the controlled term ‘unaccompanied minor’ in all three databases.
Three reviewers (AB, BS and JKvH) independently screened all search results and systematically reviewed the retrieved records by applying the eligibility criteria (box 2).
Study selection criteria
Study inclusion criteria, grading and classification
Publication type:
Studies: observational, retrospective, prospective
Language: published in English
Study population:
Refugee children from Africa, Asia or the Middle East
Age: reported results specific to children or adolescents (0–18 years)
Medical screening on children’s entry in reception countries
Sample size: minimum of 25 children
Study exclusion criteria
Publication type:
Guidelines
Surveillance registration
National notifiable disease reports
Case studies
Study population
Age not clearly defined
Results of children and adults combined
Screening of adoptees
Children attending curative services
Outbreak control
Children from the Americas, Europe or the Western Pacific
Mental disorders in refugee children
All articles identified as relevant by all three researchers were reviewed in full by two researchers (AB and BS) to determine whether they met the inclusion criteria.
Observational studies on health status among the general population of refugee children entering reception countries were considered for inclusion in this systematic review. The inclusion and exclusion criteria are shown in box 2. Mental health disorders were excluded because such a review requires a different approach. Studies were also excluded if they reported on prevalence rates among high-risk populations (eg, children whose health status was checked during hospital admission, screened during outbreaks or selected for screening through contact tracing (eg, hepatitis B and active TB)). The selection process is outlined in a flowchart in figure 1.

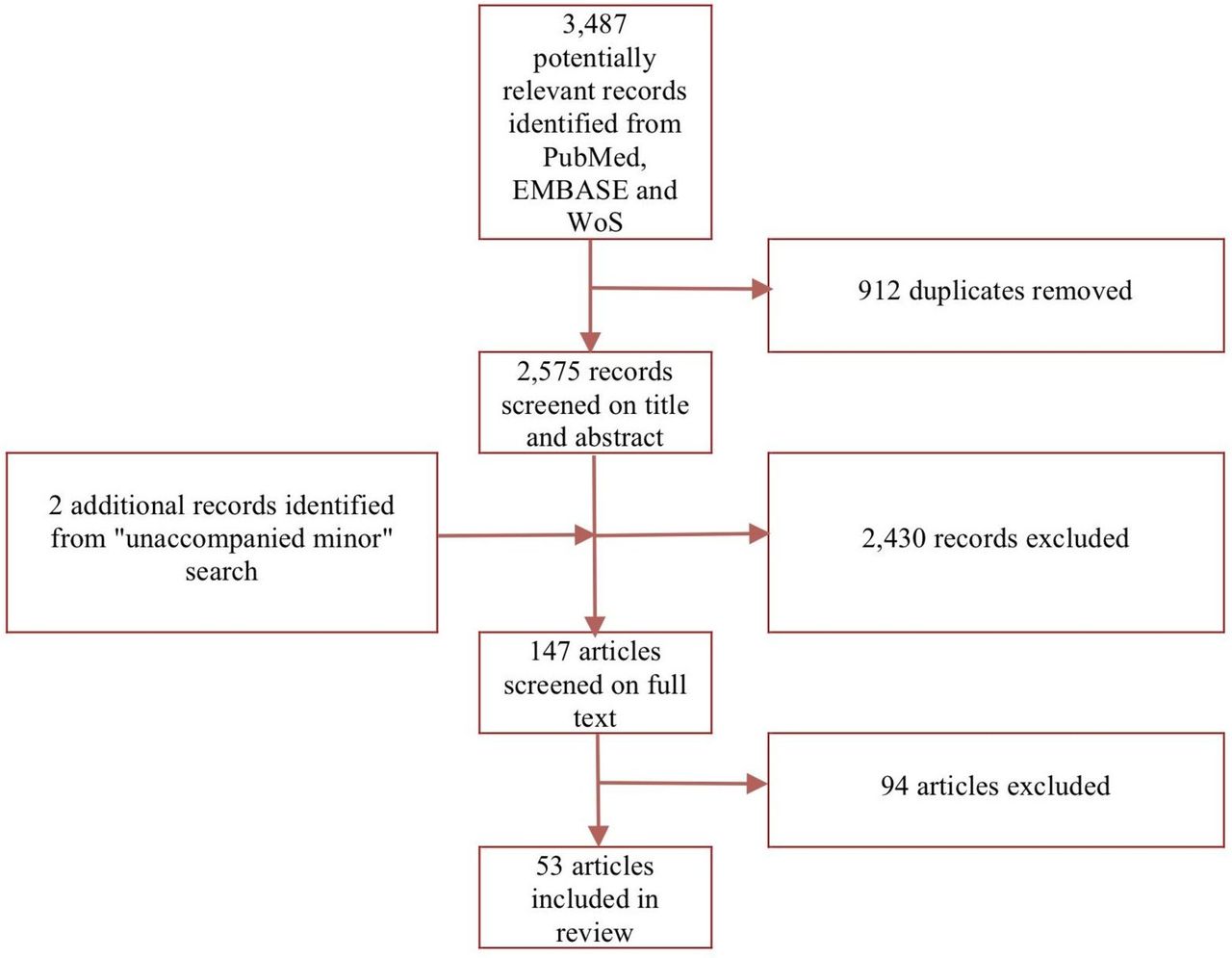{kind=link}
Flowchart selection process. WoS, Web of Science.
All selected studies were qualitatively assessed by applying a checklist of methodological quality adapted from the Dutch Cochrane Centre (see online supplementary tables S1 and S2). The representativeness of study data was assessed for all studies conducted among minority groups (including ethnic minorities) or in specific locations (see online supplementary table S2).
Supplemental material
Data analysis
We extracted the following types of data from each article: study characteristics (eg, study type and country), participant characteristics (eg, age, age range and region) and one or more of several tests (including laboratory tests and cut-points, ie, those for anaemia, genetic disorders of the red blood cells, infectious diseases, growth and nutrition, and vaccination status). Descriptive analyses and separate prevalence rates were performed using IBM SPSS V.23. All eligible articles were subjected to a meta-analysis. Prevalence rates according to health status and country of origin were also meta-analysed. A Freeman-Tukey double arcsine transformation of prevalence data was applied before pooling and back-transforming the results. A random effects model was used for all pooled prevalence rates. Forest plots were created to show the prevalence of each study and overall pooled prevalence (online supplementary file 1). Meta-analyses were conducted in R V.2.2 (Ref: R Core Team (2017). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL: https://www.R-project.org/).
Supplemental material
Results
Our systematic review included 53 articles that, when combined, conducted research on a total of 223 037 refugee children who entered one of nine reception countries from a point of origin in either Africa, Asia or the Middle East (table 1). The highest number of reports were available from the USA (n=26). Data from five European countries accounted for a total of 13 studies. Most data were available from children who originally lived in Asia or Africa. When available, data from Africa were divided into two regional blocks (ie, North African countries and sub-Saharan countries).
Reception countries of refugee children
Some articles reported on a single condition seen in refugee children, while others reported on screening procedures related to several conditions at once (table 2).
Regions of origin, reception countries and reported conditions of refugee children
Estimates of the prevalence rates for health conditions among refugee children arriving in Australia, Canada, Germany, Malta, New Zealand, Spain, the Netherlands, the UK and the USA are presented in table 3. We found 14 studies that reported on anaemia, with a pooled prevalence rate of 14%. The global pooled prevalence rate for chronic HBV is estimated at 3%. Most data on infectious diseases originated from national screening programmes for TB. Latent TB was found to be highly prevalent among refugee children. This overview also showed that one-third of refugee children had intestinal infections. Data on growth, nutrition and micronutrient deficiencies revealed that a high percentage of children were suffering from vitamin D deficiencies.
Estimated prevalences (%) and 95% CI (%) of selected conditions among refugee children 0–18 years from all regions on entry in reception countries
Tables 4–8 present health conditions among refugee children according to their region of origin. Forest plots are presented in the online supplementary file 1.
Estimated prevalences and 95% CI (%) of anaemia and haemoglobinopathies among migrant and refugee children by region of origin
Estimated prevalences and 95% CI (%) of infectious diseases among migrant and refugee children by region of origin
Prevalence of hepatitis B (HBsAg+) in refugee children from Asia by age and CI (%)
Estimated prevalences and 95% CI (%) of micronutrient deficiencies, growth and EBLL among migrant and refugee children by region of origin
Estimated prevalences (%) and 95% CI (%) of immunity for vaccine preventable disease among migrant and refugee children by region of origin (references online)
Anaemia and genetic disorders of the red blood cells
The estimated prevalence of anaemia according to region is presented in table 4. African refugee children under the age of 19 constituted the population most affected. The prevalence of anaemia was found to decrease with age; consequently, children under five were the most prone to anaemia.3 Adolescents from Syria were the least affected. Data on HbP were scarce and represented a wide variety of HbP (eg, sickle cell disease, sickle cell trait, thalassemia and G6PD).
Infectious diseases
Estimates on the burden of infectious disease by region are presented in table 5. The rate of chronic HBV among refugee children was based on 16 reports representing a total of 19 196 subjects. We also divided this rate according to age group. HBsAg seroprevalences among refugee children originating from Africa, Asia and the Middle East are reported in table 6. The highest rates of prevalence were found in African countries, with a higher intermediate endemicity (HBsAg prevalence 5%–7.99%) in sub-Saharan Africa. On average, children from the Asian region had a lower intermediate endemicity (HBsAg prevalence 2%–4.99%). HBsAg seroprevalences in Asia increased with age (table 6). Higher intermediate endemicity was found in children originating from Asia in the 12–≤19 age group. The lowest rate of endemicity was found in children from the Middle East (HBsAg prevalence≤2%). Based on the only available report, the highest endemicity of chronic HCV was found in Africa. Positive serology can be an indicator for both past or active infection and requires further evaluation. Results from three of the four studies on HIV indicated that no participating children were HIV positive. While refugee health assessments are widely implemented in the USA, testing on HIV is not routinely performed in children under the age of 15. Since 2010, HIV testing has only been performed among refugees suspected of the infection.
Data on active TB among refugee children were available from national screening programmes in the USA and the UK. For the majority of articles, data were presented as a single group and could not be broken down by age or traced to the child’s region of origin. An age breakdown was thus not possible. The highest prevalence of latent TB (16%) was found in children originating from sub-Saharan Africa. This prevalence increased with age. A high endemicity for schistosomiasis and Strongyloides seroprevalence was found in African children, mainly those originating from the sub-Saharan region. Positive serology can be a sign of past or present infection. The 15 studies on intestinal infections were conducted among a total of 12 723 refugee children. Here, an estimated 31% were infected with at least one pathogen. The main reservoir of intestinal infection was found in U5 children.
Refugee children bound for resettlement in the USA are given presumptive treatment. This contributes to a significant reduction in the prevalence of helminthiasis according to studies conducted on refugees after arrival in the USA. Refugee children from Africa showed the highest prevalence of malaria parasites.
Growth, nutrition, and micronutrient deficiencies
Up to 70% of all children from the Middle East that were studied were found to be 25-hydroxyvitamin D insufficient. Adolescents exhibited the highest prevalence of this insufficiency. Poor nutrition was evident through the presence of both underweight and overweight refugee children. A total of 11% of refugee children were reported as overweight, while 6% were classified as obese (table 7).
Discussion
This systematic review showed that refugee children entering Australia, Canada, Germany, Malta, New Zealand, Spain, the Netherlands, the UK and the USA face considerable health risks. Various factors influence the risk of disease in this population, including the lack of access to antenatal screening, vaccination programmes and healthcare in addition to political instability, war, poverty, poor hygiene and insufficient nutrition in their countries of origin. This study revealed the heterogeneous nature of the population of refugee children as demonstrated by the wide variation in the estimated prevalence rates of a range of health conditions.
The global prevalence rates of chronic hepatitis found by Schweitzer et al are in line with this study’s findings, which indicate that children originating from high-prevalence countries should be considered as at higher risk than children born in reception countries.9
There is a wide variety of national policies for screening refugee children on arrival.17 Policy statements emphasise the importance of multisector collaboration and child rights-based approaches.18
The European Association of Paediatrics has developed a practical, consensus-based recommendation for providing medical care to refugee children in Europe.19 Several clinical guidelines have been designed to address the health needs of both immigrants and refugees. The European Commission has developed a health assessment guideline for refugees and migrants entering European countries, including a section on child health and development.20 The US Centres for Disease Control and Prevention has similarly developed screening guidelines for immigrants (including refugee children) that are unique to each country of origin.21 Australian guidelines focus on infectious and non-infectious diseases.22 Canada has also established extensive guidelines for the general refugee population to cover four areas of screening (infectious disease, mental health, chronic and non-communicable disease, and reproductive health).23 The Canadian Paediatric Society has likewise tailored these guidelines based on the country of origin when dealing with children.24 There are also countries with voluntary upon-entry medical screening for refugee children. A wide variety of practices are implemented in these cases, most of which are based on fragmented and sometimes limited experience or expert opinion.
Infectious diseases have traditionally been the priority of health assessment of refugee children. Due to the shift in disease burden in refugee populations, the focus of the health assessment of refugee children has moved towards early detection of more chronic and lifestyle conditions such as obesity.25
Decisions on how, for whom and when to extend health assessments with additional tests do not solely depend on estimated prevalence rates and the probabilities of developing certain health conditions but also on outside practicalities. These include national budgets, cost-effectiveness, the reversibility of certain conditions, minority access to health systems and knowledge of health conditions among healthcare workers.
The question of cost-effectiveness is an issue that can only be answered when data specifically for refugee children are available. Veldhuijzen et al proved that adult refugee screening programmes for chronic HBV were cost-effective when the goal was to improve outcomes through early detection and treatment.26 Usemann et al stated that LTBI screening is cost-effective if progression rates of 5% and higher from latent to active TB are present in populations with an LTBI prevalence of 14%.27
Ethical questions surrounding screening programme for vulnerable groups must be considered. The screening criteria originally laid out by Wilson and Jungner provide a widely accepted framework for screening programmes.28
Another factor influencing the successful implementation of a comprehensive health assessment is the ability of healthcare professionals to provide culturally competent care. This includes ensuring the familiarity of healthcare providers with the culturally dependent presentation of symptoms and working to augment the fragmented or limited knowledge of the health risks and specific (tropical) diseases seen in refugee children.29
Some conditions may spontaneously resolve after the migration process, when children are no longer continuously exposed to infectious diseases and when they receive access to proper micronutrients. However, Penrose et al showed that vitamin D levels worsened after refugees resettled in Western countries.30
Refugee children and their families are known to have poorer access to healthcare facilities than other groups.29 Several studies have underlined the importance of professional translators when attempting to improve medical outcomes among refugee children.31 32 Many refugees are already familiar with screening processes such as the premarital test for β-thalassemia.8 Brandenberger et al underlined in their review the three key challenges in healthcare delivery for refugees and migrants: communication, continuity of care and confidence.33
Issues such as granted access to care, follow-ups, economic aspects, feasibility and sustainability also need to be addressed before implementing an extended health assessment. These are beyond the scope of this systematic review. Rigorous qualitative evaluations of all children identified with a health condition should also be conducted to ensure they receive high quality care.
Strengths and limitations of this systematic review
One strength of this systematic review was the overwhelming amount of population-based data that were available for use when analysing refugee children. However, the heterogeneity of their populations was the main limitation of this review. Unpredictable and fluctuating refugee streams and the ever-changing demographics in their countries of origin were also major limitations. The data do not necessarily reflect the current situations of conflict in the Middle East and Northern Africa, which cause rapid changes in refugee flows. The representativeness of the studied samples was also a major limitation. Therefore, we used the term estimated prevalence to describe our results. Thus, there may have been underestimates or overestimates. Prevalence rates may also vary due to introduction of new vaccination campaigns as evidenced by the declining prevalence of HBV over the last decade. We realise that our focus on English literature meant that relevant studies published in other languages would be missed.
Conclusion
Refugee children have considerable health risks on entry in reception countries. Thus, their health needs may be inadequately addressed. The results of this systematic review could be incorporated in multidisciplinary guideline development for comprehensive health assessments of refugee children tailored to the individual health needs of these children by considering their specific health risks, including those related to preflight conditions in their home countries and migration history.
This systematic review showed that we should consider a transition towards a child health-needs approach. A paradigm shift that places focus on child health and development will help this vulnerable group of children integrate into their new environments. This is critical from a governmental perspective considering many refugee children will ultimately be granted residency. Targeted health assessments on entry will assist them in gaining better access to healthcare while facilitating their familiarisation with healthcare rights. We hope this systematic review will inspire policy makers in the public health sector to pivot from national programmes designed to control infectious diseases towards health assessment procedures that focus on child health needs for the betterment of this vulnerable group of children.
References
Footnotes
Contributors AB, BS and JKvH performed the literature search. AB and BS compiled the tables (including the quality table). AB and MWH analysed the data. AB wrote the first draft of the paper. JKvH, BS, MCP and JBvG critically reviewed the manuscript and provided suggestions. AB finalised the manuscript. All authors have read and approved the final version of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.