Article Text

Abstract
Background Bronchiolitis is a major cause of admission to hospital in children. Non-invasive ventilation (NIV) support with continuous positive airway pressure (CPAP) or high-flow nasal cannula (HFNC) oxygen is routinely used for infants in the UK with bronchiolitis.
Objective To establish UK paediatric practice regarding management of bronchiolitis, and to explore issues pertinent to the design of a potential future randomised controlled trial of NIV.
Design Screening logs were completed in hospitals in England capturing information on paediatric bronchiolitis admissions. An online national survey of clinical practice was disseminated to healthcare professionals (HCPs) across the UK to ascertain current management strategies.
Results Screening logs captured data on 393 infants from 8 hospitals. Reasons for admission were most commonly respiratory distress and/or poor fluid intake. Oxygen was administered for 54% of admissions. Respiratory (CPAP and HFNC) and non-respiratory support administered varied considerably. The national survey was completed by 111 HCPs from 76 hospitals. Data were obtained on criteria used to commence and wean NIV, responsibilities for altering NIV settings, minimum training requirements for staff managing a child on NIV, and numbers of trained staff. Most centres were interested in and capable of running a trial of NIV, even out of normal office hours.
Conclusions Respiratory and non-respiratory management of bronchiolitis in UK centres varies widely. A trial of HFNC oxygen therapy in this group of patients is feasible and HCPs would be willing to randomise patients into such a trial. Future work should focus on defining trial eligibility criteria.
- neonatology
- therapeutics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Bronchiolitis is one of the the most common causes of hospitalisation in infancy.
Non-invasive ventilation and specifically high-flow nasal cannula oxygen therapy is increasingly used for children with bronchiolitis based on limited evidence in the UK.
There is widespread support among paediatricians in the UK for a trial of non-invasive ventilation to guide UK practice.
What this study adds?
Respiratory and non-respiratory management of bronchiolitis in UK centres varies widely.
A trial of high-flow nasal cannula oxygen therapy is feasible and healthcare professionals would be willing to randomise patients into such a trial.
Introduction
Bronchiolitis is a major cause of admission to hospital in children.1 2 Between 2004 and 2012, 8172 children under the age of 1 year were admitted to a paediatric intensive care unit (PICU) for bronchiolitis in England.3 From 2004 to 2011, the overall average PICU admission rate increased by 1.8% each year.3
Bronchiolitis management is centred on oxygen therapy for hypoxia, respiratory support and good hydration. Early use of non-invasive ventilation (NIV), such as continuous positive airway pressure (CPAP) or heated humidified high-flow nasal (HFNC) oxygen (O2), may have an impact on outcome by avoiding disease progression.4 There has been an increase in the use of HFNC in routine clinical practice for moderate-to-severe bronchiolitis; however, until recently, there has been little evidence to guide practice, and there have been no studies using NHS patients from the UK.5 6 Recently, a number of reports have raised concerns regarding its cost effectiveness in bronchiolitis.7
The objectives of this study were to assess current UK practice regarding bronchiolitis management in terms of the type of NIV methods used and the criteria for commencing and weaning NIV. We also wished to explore issues pertinent to the design of a potential future randomised controlled trial (RCT) of NIV. This study formed part of a larger research project (Non-Invasive Ventilation for the Management of Children with Bronchiolitis: a feasibility study (NOVEMBR)).8
Methods
A point-prevalence study, using paper screening logs of paediatric hospital admissions with bronchiolitis, was prospectively completed, by research nurses from district general hospitals and paediatric tertiary centres hospitals across England. The logs gave guidelines for completion and captured: patient age, referral route, demographic and clinical risk factors, reasons for admission, treatment interventions during admission, method of O2 delivery and amount of O2 (if any), and length of hospital stay. In total, 14 hospitals were approached for participation of which eight responded (five district general hospitals and three paediatric hospitals; see online supplemental list 1 for a list of the hospitals). The logs were circulated in two waves: the first wave included five hospitals and ran from 12 December 2016 to 12 January 2017; the second wave included three different hospitals from 11 December 2017 to 13 January 2018. The same log was used for all hospitals; repeat sampling was not used. Data on all patients admitted with a diagnosis of bronchiolitis during these time periods to these hospitals were captured.
Supplemental material
In addition, an online national survey (online supplemental material) was developed by the study management group to explore current practices of HCPs when managing bronchiolitis. The survey was piloted among clinical members of the Study Management Group, which comprised PICU, respiratory and general paediatricians, paediatric nurses and research nurses. Amendments made from the piloting process were improvements to the clarity and understanding of the survey by changes to some of the language. The survey was disseminated to lead paediatricians at all paediatric centres in the UK through the National Institute for Health Research Clinical Research Network (CRN) Coordinating Centre to Specialty Cluster Office for Children and Local CRNs, and through the General and Adolescent Paediatric Research Collaborative UK and Ireland. The lead paediatricians were asked to complete the survey themselves or to pass it on to whoever they considered most appropriate. It was conducted online between 29 September 2017 and 31 January 2018. Respondents were asked to report their job title and give information about their hospital including: the number of estimated paediatric bronchiolitis admissions, type of NIV interventions used and who administers them, criteria for initiating and weaning CPAP and HFNC, availability of local bronchiolitis care pathways and lastly, questions to determine the acceptability to HCPs of running a clinical trial. Completion of the survey was deemed consent to participate.
Data from both the screening logs and the online national survey were summarised using descriptive statistics. Where questions were missed or responses ‘Not known’, percentages were derived using denominators for those who gave an answer only.
Advice from the HRA was sought and it was confirmed that ethical approval was not required for the online survey. Approval was not required for the screening exercise as only anonymous data were collected.
Patient and Public Involvement (PPI) was not included for this component of the NOVEMBR study since the aim was to ascertain current practice amongst HCPs.
Results
Screening logs
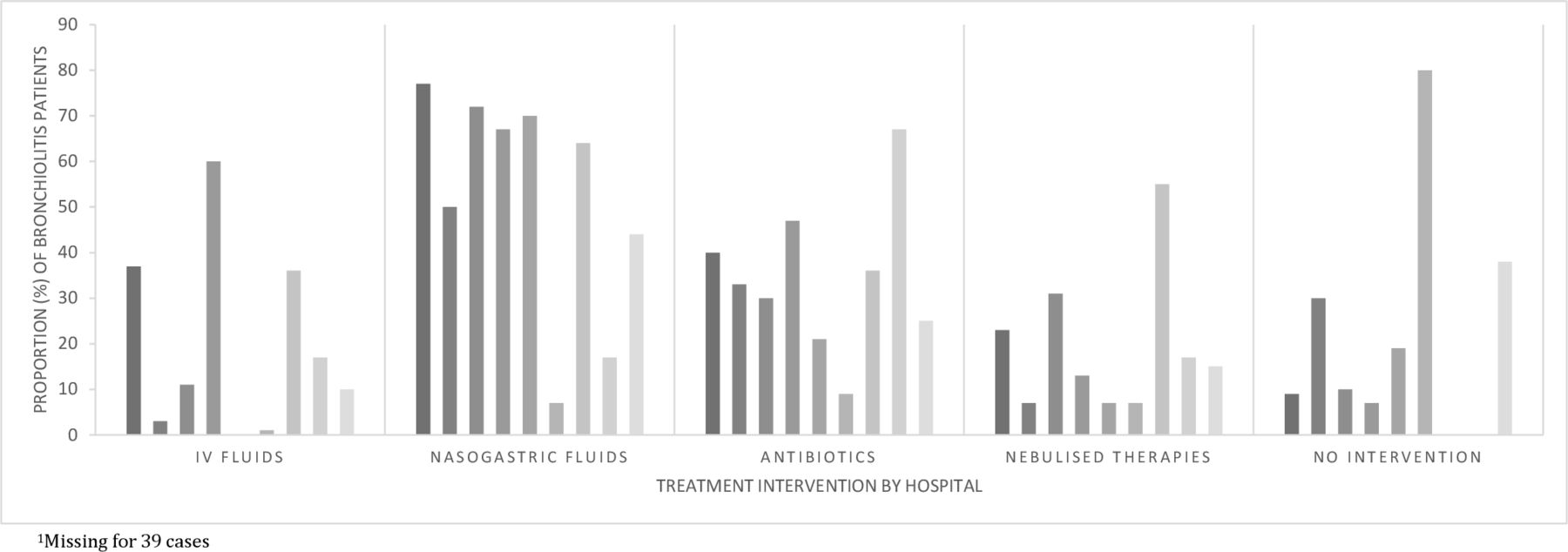
Table 1 gives a summary of the screening data. Three hundred and ninety-three patients were screened at eight hospitals across England (online supplemental list 1). Data by hospital are presented in online supplemental table 1. The greatest proportion (139/357, 39%) were admitted in the afternoon and early evening (14:00–20:00). Median age at admission was 14 weeks (IQR: 8–29) and median length of hospital stay was 2 days (IQR: 1–3). Most referrals were via emergency departments (246/391, 63%) or from general practitioners (99/391, 25%). It was possible for multiple reasons for admission to be selected for each patient; among the most frequent, over half (203/392, 52%) reported difficulty with breast feeding/inadequate oral fluid intake, 36% (142/392) other respiratory problems, including cough and increased work of breathing, 31% (121/392) severe respiratory distress and 27% (106/392) of children looked seriously unwell to a HCP. Commonly reported risk factors for hospital admission included age less than 3 months (165/357, 46%) and/or prematurity (89/357, 25%); 34% (120/357) reported no risk factors. Non-respiratory interventions included: nasogastric fluids (157/354, 44%), antibiotics (87/354, 25%), nebulised treatments (52/354, 15%) and intravenous fluids (37/354, 10%); 38% (134/354) reported no treatment intervention. There was considerable variation across hospitals: nasogastric fluids use ranged from 17% to 77% of infants, antibiotics from 9% to 67%, nebulisers from 7% to 55% and intravenous fluids from 1% to 37% (figure 1). Oxygen was delivered to 191 (54%) patients. Multiple methods for O2 delivery could be selected; methods reported were low-flow nasal cannula (103/191, 54%), rebreathe mask (42/191, 22%), head box with humidified O2 (25/191, 13%), HFNC (52/191, 27%), CPAP (18/191, 9%) and intubation and ventilation (21/191, 11%).
Screening data

Screening responses—treatment interventions across hospitals.
National online survey of current practice
The survey was accessed by 123 individuals. Twelve (9%) completed demographic details only and were excluded from the summaries; the remaining 111 (91%) responders were from 76 hospitals (online supplemental list 2). The majority (83/111, 75%) of respondents were from district general hospitals; 25% (28/111) were from paediatric tertiary centres. According to the Royal College of Paediatrics and Child Health workforce document published in 2019, there are 189 paediatric centres with inpatient facilities in the UK of which 35 are considered specialist (tertiary) centres.9 Respondents were either consultants (92/109, 84%) or nurses (12/109, 11%, table 2).
Survey participant/hospital demographics
Almost half (47%, 38/81) of respondents stated that the estimated annual number of paediatric bronchiolitis admissions to their hospital with a length of stay of at least 1 day, was between 101 and 200, and 30% (24/81) estimated between 51 and 100. The majority (71/84, 85%) of respondents stated local bronchiolitis care pathways and/or guidance were available to them; 86% (75/87) reported the criteria for starting O2 was SpO2 <92%. Six respondents (6/88, 7%), from separate hospitals, reported the ability to send home children with bronchiolitis on O2.
CPAP/HFNC
More respondents reported being able to deliver O2 on paediatric wards by HFNC (73/86, 85%) than CPAP (49/86, 57%); 55% reported the ability to deliver O2 using both treatment modalities. On High Dependency Units (HDU), the ability to deliver O2 using either was similar (HFNC, 70/73, 96%; CPAP, 64/73, 88%).
The modal estimate of infants with bronchiolitis that did not require O2 on admission reported by respondents was 11%–20%, whereas the estimate of infants that did require O2 was 61%–70%. Although the modal estimate of infants treated with CPAP or HFNC was similar (0%–10%), the variation was more marked for HFNC, with some respondents estimating that up to 80% of patients requiring NIV in their centres would be treated with HFNC, compared with a maximum of 40% estimated to be treated with CPAP (online supplemental table 5).
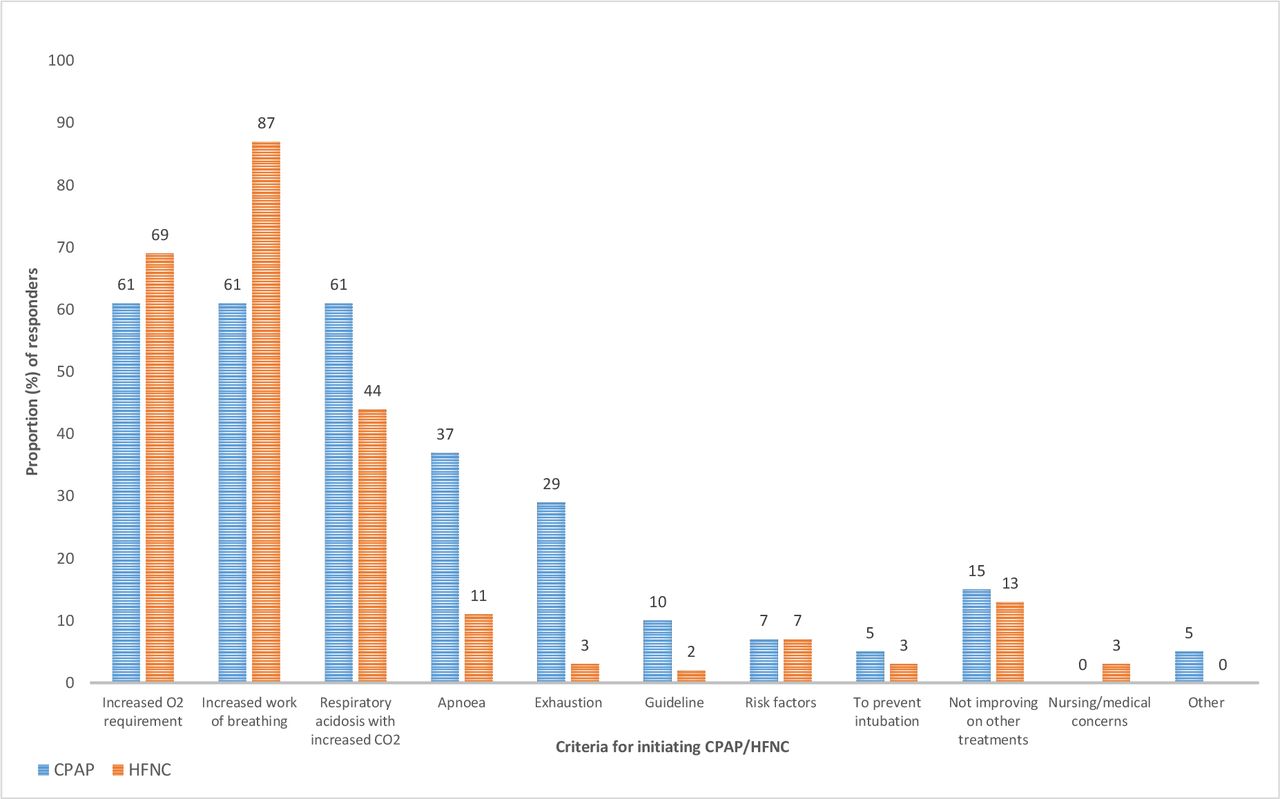
Apnoea, type 2 respiratory failure, exhaustion and the child not improving on alternate therapies (mostly HFNC) were more commonly cited as criteria to start CPAP compared with HFNC (figure 2, online supplemental table 3); HFNC was started for increased work of breathing more often than CPAP. Correspondingly, resolved apnoea, and improved C02/respiratory acidosis were more commonly cited as criteria for weaning CPAP compared with HFNC. Responsibilities for altering CPAP/HFNC settings lay predominantly with the nursing staff, who were responsible in 40% (23/57) of cases on CPAP compared with 77% (46/60) of cases on HFNC. Minimum training requirements for staff to manage a child on CPAP/HFNC were similar for both methods and included: annual attendance of in-house training packages with and without clinical competency assessments, attendance to ad hoc training sessions run by equipment manufacturers and high dependency courses.
{kind=link}
{kind=link}
Survey responses—criteria for initiating continuous positive airway pressure (CPAP) compared to high-flow nasal cannula (HFNC).
Acceptability of a trial
Most respondents (34/41, 83%) reported that it would be possible to run a clinical trial evaluating NIV treatment approaches in bronchiolitis even out-of-hours at their hospitals (online supplemental table 4). Forty respondents suggested at least one barrier to undertaking such a trial. Barriers included: current medical/nursing staff workload (15/40, 38%), availability of equipment (7/40, 18%), lack of research nurse support (4/40, 10%) and lack of adequately trained staff to undertake a trial (3/40, 8%). Correspondingly, 47 respondents suggested at least one enabler to undertaking a trial: having adequate medical, nursing and research nurse support (24/47, 51%), good training and education about any trial (8/47, 17%) and importantly, having access to extra equipment (8/47, 17%). Sixty per cent (47/78) estimated that 1–5 HDU beds would be available in winter.
Respondents at 72% of sites reported always having one or more GCP trained doctor on every shift. Similarly, respondents at 45% of sites reported that their site had one or more GCP trained nurse on every shift.
Discussion
In this prospective observational study of bronchiolitis admissions, large numbers of children (particularly young infants approximately 3 months of age) were hospitalised with this condition but generally for only a few days. Many (46%) did not require oxygen during their admission, but in those who did, the method by which it was administered varied widely; this was particularly so for those requiring NIV. Despite publication of The National Institute for Health and Care Excellence (NICE) guidelines on bronchiolitis in 2015,3 there remains considerable variation in other aspects of management.
This study provided the opportunity to compare survey responses from a large number of UK paediatric HCPs with screening log data on actual bronchiolitis admissions to secondary and tertiary centres. Survey responses overestimated the proportion of children requiring O2 on admission compared with screening log data, and although modal estimates of CPAP usage were broadly in line with actual usage, estimates of HFNC usage underestimated actual usage. In interpreting these results, it should be acknowledged that the screening log data were based on admissions to only eight paediatric centres, and that there was a wide range of estimates of percentages of children treated with O2 and with NIV (particularly HFNC). It may also be the case that the screening results differ between district general hospitals and paediatric tertiary centres; however, our sample size did not permit such a comparison.
We compared reasons for starting and weaning NIV. Apnoea, type 2 respiratory failure, exhaustion and the child not improving on alternate therapies (mostly HFNC) were more commonly cited as criteria to start CPAP. Correspondingly, resolved apnoea, and improved C02/respiratory acidosis were more commonly cited as weaning criteria for CPAP than HFNC. The overall consistency of approach to starting and weaning NIV suggests the need for a consensus-based clinically pragmatic protocol for any future trial, and that agreeing criteria and a protocol to initiate and wean NIV across sites in a future trial is feasible. Furthermore, such criteria have already been adopted for a UK-based pragmatic trial in critically ill children on both stepping up and stepping down non-invasive respiratory support.10
Based on our findings, we would question whether it is currently feasible for a HFNC versus CPAP trial to be undertaken outside of PICUs and high-dependency units in the UK. This is primarily for reasons of capacity/capability, with many centres unable to support the use of CPAP on general paediatric wards and also given the recent funding and start of the FIRST-ABC (First-line support for Assistance in Breathing in Children) trial which is examining the non-inferiority of HFNC compared with CPAP.10 However, a trial to assess the clinical effectiveness of HFNC versus standard oxygen therapy (‘standard’ agreed a priori) is feasible and one which many general paediatricians would likely support. A key issue for any such trial would be eligibility criteria. NOVEMBR and recently published RCTs of NIV for bronchiolitis suggest that eligibility cannot be based solely on the need for oxygen.5 6 We have shown here that although over half children hospitalised with bronchiolitis are hypoxic on admission, most do not require O2 for long (under 24 hours), do not deteriorate that frequently, and do not have prolonged inpatient admissions. Even for those hypoxic children at high risk of severe bronchiolitis (ie, those less than 3 months of age or born prematurely), the median (IQR) length of stay in hospital was only 2 (1–3) days. Key eligibility criteria for any future trial will likely have to include both need for O2 and increased work of breathing, and take into account risk factors such as young age/prematurity. It is these infants for whom HFNC likely has the biggest potential to demonstrate clinical and cost effectiveness. A retrospective cohort study published in 2018 identified predictors of escalated care in bronchiolitis and used these to derive a risk score to outline higher risk patients; validation of such a score would be beneficial.11
The screening logs highlighted a large variation in the frequency with which various non-respiratory interventions were used in children with bronchiolitis. Variation on this scale has previously been reported between countries, but not to our knowledge within the UK.12 When designing potentially large multicentre trials of NIV for children with bronchiolitis, an appreciation of this sort of variation in practice may be needed when planning patient recruitment per site and trial acceptability.
There were two limitations of note, the first being that in the survey multiple responses from the same hospital could have inflated the proportions for certain responses. To check the validity of our results, we looked at the results with each hospital included only once for each response level (online supplemental tables 2-4) and found that the proportions were similar. The second limitation was that participants from the same hospital occasionally reported different answers, which is likely due to different perspectives depending on the job roles of the respondents; however, sample sizes prevented us from exploring differences between HCP subgroups (ie, nurses from general paediatric wards and those from HDU).
We have established that there is a wide variety of practice across the UK in the respiratory and non-respiratory treatments given to infants with bronchiolitis. Our results also suggest that a trial of NIV is feasible and that HCPs would be willing to randomise patients into an NIV trial. Future work should now focus on defining the eligibility criteria for such a trial.
Supplemental material
Acknowledgments
The authors would like to acknowledge the healthcare professionals who participated in the screening log and survey of national practice. They also would like to thank the funder, the NIHR Research for Patient Benefit Programme.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CvM and PM conceived the study. CvM, PM, RF and KW designed the study. EB, MP, KT, VC and DL were members of the study management group. AR-H analysed the data. AJ supervised data analysis. AR-H, APJ and PM drafted the manuscript. All authors reviewed and provided comments on the manuscript.
Funding This research was funded by the National Institute for Health Research (NIHR), Research for Patient Benefit (RfPB) Programme (Grant Reference Number PB-PG-1014-35081).
Disclaimer Views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests CvM was an invited speaker at a meeting sponsored by Fisher & Paykel. PM sits on an independent data monitoring and safety committee of an early phase trial of an antiviral treatment for bronchiolitis funded by Pulmocide and as an advisor for antiviral trials for bronchiolitis funded by Janssen and Alios. RF has served on independent data monitoring and safety committees of early phase trials in bronchiolitis funded by Ablynx and on a clinical endpoint committee for an RSV vaccine trial funded by Janssen.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The datasets generated are available from the corresponding author on reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.