Article Text

Abstract
Objective Whether hypoglycaemia incidentally detected during intercurrent illness in children requires an endocrine workup remains controversial. This study aimed to determine the yield of conducting a diagnostic evaluation in this setting and to compare clinical and biochemical features between patients ultimately diagnosed with a hypoglycaemic disorder and those who were not.
Design Single-center, retrospective review of children referred to endocrinology between January 2013 and December 2018 for evaluation of hypoglycaemia (defined as plasma glucose<3.9 mmol/L (<70 mg/dL)) in the setting of acute illness.
Results 145 patients met eligibility criteria. A hypoglycaemia disorder was identified in 12 patients (8% of the cohort, 17% of those who underwent a diagnostic fast). There were no cases in which diagnosis was established in the absence of a diagnostic fast. Characteristics associated with identifying an underlying disorder included younger age (1.03 years (IQR: 0.05–1.54) vs 2.18 years [IQR: 1.29–3.99], p<0.001), higher bicarbonate level (22±5.5 mmol/L vs 16±3.6 mmol/L, p<0.001), lower frequency of elevated plasma or urine ketones (25% vs 92%, p=0.004) and lower frequency of other documented medical problems (17% vs 50%, p=0.03).
Conclusions The yield of diagnostic evaluation among children with incidental detection of hypoglycaemia in the setting of illness is not insignificant. We thus recommend that all children with hypoglycaemia in the setting of illness undergo guided diagnostic evaluation. Younger age and absence of ketosis and acidosis at presentation may serve as useful predictors for establishing a diagnosis. Future studies are needed to confirm these findings.
- Endocrinology
Data availability statement
Data are available upon reasonable request. Data that support the findings of this study are included in this article and its online supplemental material file. Further enquiries can be directed to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The prevalence of undiagnosed hypoglycaemia disorders among children seen in the emergency department for any clinical reason has been reported as 10%–28%. During illness, oral intake in children is often reduced. In this setting, incidentally hypoglycaemia is often attributed to prolonged fasting. Determining whether children with hypoglycaemia detected during illness require a dedicated endocrine evaluation has been limited by a paucity of data.
WHAT THIS STUDY ADDS
In this cohort, 8% of children who presented with hypoglycaemia in setting of illness were found to have an underlying hypoglycaemia disorder. Underlying hypoglycaemia diagnoses were only established in those children who underwent a comprehensive evaluation including diagnostic fast. Younger age, higher bicarbonate level and lower ketones at presentation were associated with establishing a hypoglycaemia diagnosis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
All children with hypoglycaemia detected in the setting of acute illness should undergo guided diagnostic evaluation.
Introduction
Incidental detection of hypoglycaemia during childhood illness commonly occurs following prolonged starvation, in which glucose utilisation exceeds glucose supply. Rarely, it may be the initial presentation of an underlying hypoglycaemia disorder wherein missing the diagnosis carries a high risk of harm. The reported prevalence of undiagnosed hypoglycaemia disorders among children seen in the emergency department for any reason ranges between 10% and 28%.1–3 However, these studies were not limited to children presenting with acute illness. Consequently, whether children with hypoglycaemia detected during acute illness require an endocrine workup remains controversial. We sought to evaluate the yield of conducting an evaluation when hypoglycaemia occurs in this setting and to describe the clinical and biochemical features of those children ultimately found to have underlying pathology.
Materials and methods
A retrospective review was conducted of children referred to endocrinology for evaluation of hypoglycaemia (plasma glucose<3.9 mmol/L (<70 mg/dL)) in the setting of acute illness at Children’s Hospital of Philadelphia (CHOP) between January 2013 and December 2018. Billing records were used to obtain a list of inpatient and outpatient endocrine consults for hypoglycaemia using International Classification of Diseases (ICD) codes for ‘hypoglycaemia, unspecified’ (ICD-9 251.2 prior to October 2015, ICD-10 16.2 after October 2015). Additionally, inpatient billing records were manually searched for ‘hypoglycaemia’ as the consultation reason. Patients were included if they were <18 years of age and had both documented plasma glucose <3.9 mmol/L (<70 mg/dL) and illness symptoms (eg, fever, vomiting, diarrhoea, respiratory symptoms) at the time of presentation. Exclusion criteria included children with previously diagnosed hypoglycaemia disorders, diabetes mellitus or use of medications that can alter glucose metabolism (hypoglycaemic agents, systemic steroids, chemotherapy or beta-blockers) within 1 month of presentation. A plasma glucose threshold of <3.9 mmol/L (<70 mg/dL) was used to define hypoglycaemia in this study in keeping with established hypoglycaemia definitions,4 5 and because below this threshold, neuroendocrine responses to hypoglycaemia are activated.6 Additionally, most infants and children are able to maintain plasma glucose above this threshold after 15–18 hours of fasting.7
Demographic, clinical and biochemical data were extracted from the electronic health record (EHR). Acute illness was categorised as: gastroenteritis, isolated vomiting, isolated diarrhoea, upper respiratory infection, otitis media, fever and other. Illness categories were not exclusive; patients were included in all categories for which there were documented symptoms. Height and weight were used to calculate weight-for-length percentiles for patients <2 years of age and body mass index (BMI) percentiles for patients ≥2 years of age. Weight status was categorised as: underweight (weight-for-length/BMI <5 percentile for age), normal weight (weight-for-length/BMI ≥5 and <85 percentile for age), overweight (weight-for-length/BMI ≥85 and <95 percentile for age) and obese (weight-for-length/BMI ≥95 percentile for age). Physical examination findings of interest included dysmorphic features, hepatomegaly and signs of suggestive of hypopituitarism (midline defects, microphallus in males).
Types of hypoglycaemia evaluation performed included laboratory studies drawn at the time of presentation, non-fasting laboratory studies obtained following presentation (‘baseline evaluation’), genetic testing and diagnostic fasting studies, which were conducted as previously described (standard protocol8). Evaluations were conducted at the discretion of the provider. This was typically an emergency medicine provider at presentation. The decision to pursue diagnostic fasting studies was made solely by endocrinologists. Standard practice at our centre is to obtain baseline metabolic studies (acylcarnitine profile, total and free carnitine levels and urine organic acids) prior to performing fasting studies when there is concern for a possible fatty acid oxidation disorder. To facilitate comparison between groups, urine and blood ketone levels were combined into categories wherein positive ketones were defined as either small or greater urine ketones or blood ketones≥1 mmol/L; ketones were otherwise defined as negative.
The EHR was reviewed for additional episodes of hypoglycaemia and for endocrine or metabolic diagnoses (hormone deficiencies, disorders of insulin secretion/signalling, glycogen storage disease, disorders of gluconeogenesis and fatty acid oxidation disorders) made subsequent to the index event. Duration of follow-up was calculated from index event and last contact dates.
Statistical analysis
Categorical variables were reported as proportions. Normally distributed continuous variables were summarised using mean and SD. Median and IQR were reported for non-normally distributed continuous data. In comparing the clinical and biochemical characteristics of patients ultimately diagnosed with a hypoglycaemic disorder with those who were not, and patients who underwent a diagnostic fasting evaluation with those who did not, proportions were compared using Fisher’s exact test, t-tests were used to compare means of normally distributed data and Wilcoxon rank sum tests were used to compare medians of non-parametric data. All tests were two-sided with p<0.05 set as the threshold for statistical significance.
Results
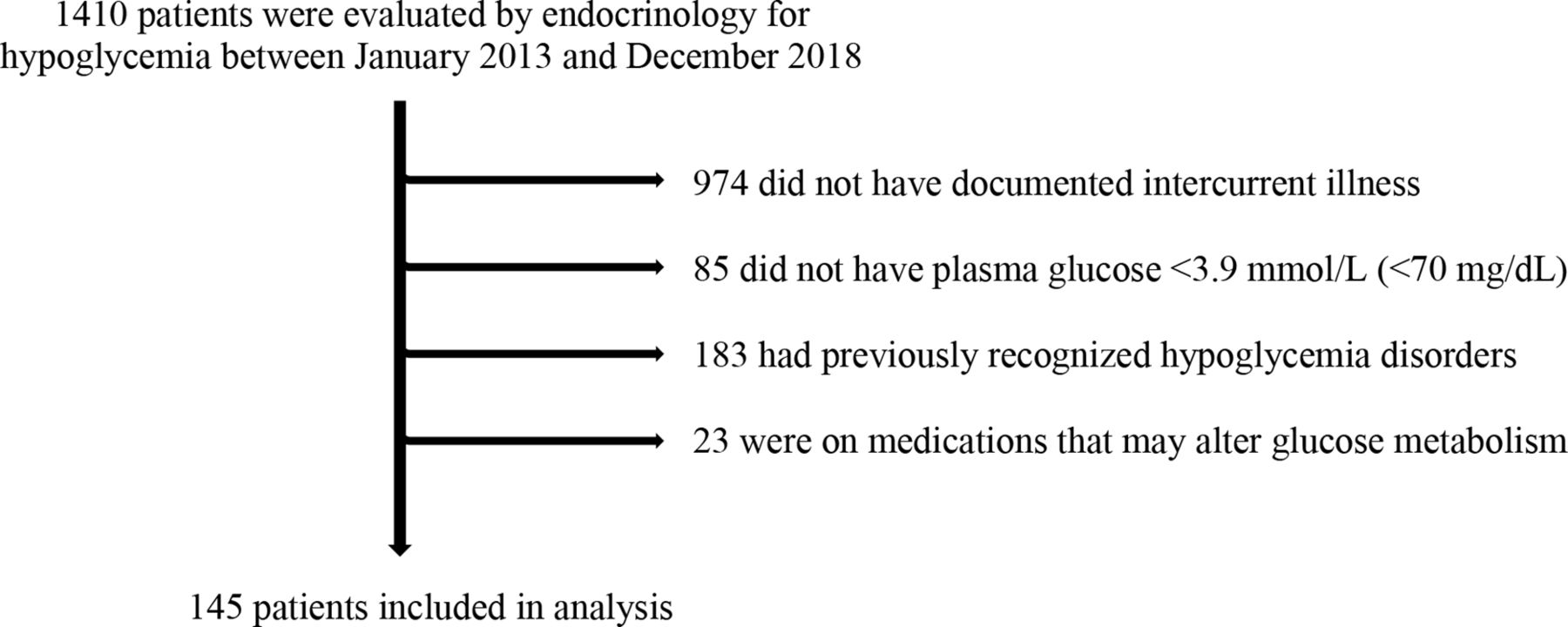
A total of 1410 patients were evaluated by endocrinology for hypoglycaemia at CHOP between January 2013 and December 2018. Of these, 145 patients met inclusion criteria, and their records were reviewed (figure 1). Characteristics of the cohort at time of presentation are summarised in table 1. Median age at presentation was 2 years and ranged from 2 days to 11 years. Abnormal findings on physical examination were uncommon. Four patients had dysmorphism, three had hepatomegaly and one had macrocephaly. No patients had documented cleft lip or palate or microphallus.

{kind=link}
Consort diagram.
Cohort characteristics
Overall, 13% of patients presented with altered mental status and 10% presented with seizure-like activity. Of the patients with a prior history of hypoglycaemia, none had previously undergone a diagnostic evaluation. Thirty-four per cent of patients had recurrent episodes of hypoglycaemia following the index event. The median follow-up duration was 27 months (range: 0 days to 7.8 years).
Evaluations conducted
Laboratory evaluations performed at any point during follow-up varied considerably. At the time of initial presentation with hypoglycaemia, urine or plasma ketones were obtained in 57% of patients, bicarbonate was obtained in 63%, transaminases were measured in 28% and cortisol was obtained in 11%. Lactate, ammonia, insulin, c-peptide, free fatty acids, growth hormone and metabolic studies (acylcarnitine profile, total and free carnitine levels and urine organic acids) were each obtained in <10% of patients. Of the patients who had laboratory evaluation beyond glucose, ketones and bicarbonate at the time of initial presentation, 50% had abnormal findings. Abnormal findings included elevated transaminases (ie, above the upper limit of normal) in 50% and elevated lactate in 18%. Cortisol was >276 nmol/L in all patients in whom it was obtained. Baseline evaluation was obtained in 59% of patients with metabolic studies performed most frequently. Baseline evaluation yielded abnormal findings in 29% of patients.
Of the 102 patients with plasma glucose <2.8 mmol/L (<50 mg/dL) on presentation, ‘critical sample’ labs including insulin, urine or plasma ketones, lactate, ammonia, cortisol, growth factors and acylcarnitine profile were obtained in 10%. Seventy per cent of patients in whom a ‘critical sample’ was obtained had symptomatic hypoglycaemia at the time of presentation.
A diagnostic fasting test was performed, either at the time of initial presentation or during a follow-up admission, in 48% of patients. Twenty-five per cent of the cohort had genetic testing performed (online supplemental table 1). Only two children had genetic testing without also undergoing a diagnostic fast.
Supplemental material
Identified hypoglycaemia diagnoses
An underlying hypoglycaemia disorder was identified in 12 patients (8%) all of whom underwent a diagnostic fast. The clinical presentation, evaluation and course of these patients are detailed in online supplemental table 2. The yield of performing a diagnostic fast in this study was 17%.
Supplemental material
Hyperinsulinism was the most frequently identified aetiology and was diagnosed in seven patients. Additional diagnoses included inborn errors of metabolism in three patients, growth hormone deficiency in one patient and impaired hepatic insulin clearance due to acute hepatic insufficiency in one patient. A final diagnosis was established in two patients in whom laboratory evaluation at presentation other than glucose, ketones and bicarbonate yielded abnormal findings. In both cases (dihydrolipoamide dehydrogenase (DLD) deficiency and impaired hepatic insulin clearance), transaminases were elevated above the upper limit of normal for age.
An underlying genetic diagnosis was suggested based on testing in four patients and included hyperinsulinism due to an autosomal dominant mutation in ABCC8, hyperinsulinism associated with Turner syndrome, isolated 3-methylcrotonyl-CoA carboxylase deficiency and DLD deficiency.
Factors associated with identifying a specific hypoglycaemia diagnosis
We compared clinical and biochemical characteristics at the time of presentation between the patients ultimately diagnosed with an underlying aetiology of hypoglycaemia and those who were not (table 2). Younger age (1.03 years (IQR: 0.05–1.54) vs 2.18 years (IQR: 1.29–3.99), p<0.001) and higher bicarbonate level (22±5.5 mmol/L vs 16±3.6 mmol/L, p<0.001) were associated with identifying an underlying disorder. Weight-for-age percentile was lower in patients diagnosed with a hypoglycaemia disorder (13.1 (IQR: 1.7–23.8) vs 31.0 (IQR: 14.0–59.5), p=0.02) but weight status (ie, weight adjusted for length/height) did not statistically significantly differ between those who were diagnosed with a hypoglycaemia disorder and those who were not. Patients diagnosed with a hypoglycaemia disorder were less likely to have elevated plasma or urine ketones at presentation (25% vs 92%, p=0.004) and were less likely to have a documented history of other medical problems (17% vs 50%, p=0.03). No statistically significant differences were observed between groups with regard to the other clinical or biochemical features assessed.
Characteristics of patients in whom an underlying aetiology for hypoglycaemia was identified versus those without a diagnosis
Since a diagnostic fast was performed in all patients who ultimately had a final diagnosis established, we evaluated whether there were any characteristics at presentation associated with conducting this evaluation (table 3). Median plasma glucose at presentation was lower in the group that underwent a diagnostic fast (2.2 mmol/L (40 mg/dL), IQR: 1.8–2.7 mmol/L (32–49 mg/dL) vs 2.6 mmol/L (47 mg/dL), IQR: 2.3–3.0 mmol/L (41–55 mg/dL), p=0.002). Additionally, the proportion of patients with presenting plasma glucose<2.8 mmol/L (<50 mg/dL) was greater among those who underwent a diagnostic fast compared with those who did not (80% vs 62%, p=0.03).
Factors associated with performing diagnostic fast
Discussion
Eight per cent of children who presented with hypoglycaemia in setting of illness were found to have an underlying hypoglycaemia disorder. Underlying diagnoses were only established in children who underwent a diagnostic fast, which was conducted in 48% of patients. The frequency of underlying hypoglycaemia disorders was thus twofold higher (17%) among those who underwent a diagnostic fast as compared with the overall cohort.
These findings are in keeping with those of White et al, who found that among children seen in the emergency department for any reason with previously unrecognised hypoglycaemia (plasma glucose<2.8 mmol/L (50 mg/dL)), 10.6% were diagnosed with a hypoglycaemia disorder.3 Diagnoses were only identified in the children who underwent diagnostic evaluation (53%), such that 20% of those who had a workup were found to have a hypoglycaemia disorder. These findings emphasise that without appropriate evaluation, children with underlying hypoglycaemia disorders may not be identified.
In a similar cohort of all comers to the emergency room in whom plasma glucose was <2.5 mmol/L (<45 mg/dL), the frequency of previously unrecognised metabolic or endocrinologic disorders among those without infectious diseases causing prolonged fasting was 11%.9 Pershad et al reported that among children 1–5 years of age seen in the emergency department with an ICD code for hypoglycaemia and a plasma glucose <2.2 mmol/L (<40 mg/dL) or <3.3 mmol/L (<60 mg/dL) with neuroglycopenic symptoms, 16% were diagnosed with an endocrine or metabolic disorder.1 Details on the evaluations conducted and proportion of patients that underwent evaluation were absent from these latter two studies. Notably, the frequency of finding an underlying hypoglycaemia disorder in our study is akin to that reported in the broader population of children seen in the emergency department for any cause, potentially suggesting that the presence of illness symptoms may be less pertinent than other clinical factors in identifying children with underlying hypoglycaemia disorders.
Weinstein et al found that 28% of children seen in the emergency department and incidentally detected plasma glucose <2.8 mmol/L (<50 mg/dL) had an undiagnosed endocrine or metabolic disorder.2 In this study, patients were prospectively recruited using software, which permitted both unbiased subject enrollment and ‘critical sample’ collection prior to correction of hypoglycaemia. This is in contrast to the present study in which the decision to obtain a ‘critical sample’ was at the discretion of the provider, typically an emergency medicine provider, and was obtained in only 10% of those with plasma glucose <2.8 mmol/L (<50 mg/dL). Reasons for the low rate of ‘critical sample’ collection are unclear. The majority of children for whom a ‘critical sample’ was obtained had symptomatic hypoglycaemia, and it is possible that prompt treatment of hypoglycaemia was prioritised over obtaining laboratory assessment in children able to tolerate oral carbohydrate whereas ‘critical sample’ laboratories were more likely to be obtained in children in whom administration of intravenous dextrose was considered. The higher diagnosis rate in the Weinstein study, in which the decision to pursue evaluation was automated and not based on provider discretion, accentuates the previously absent data to guide clinical practice in deciding which patients require further evaluation.
We found that young age and absence of acidosis and ketosis at presentation were associated with identifying an underlying hypoglycaemia disorder. When hypoglycaemia occurs in a child as a consequence of starvation (ie, during illness), the child should have concomitantly elevated plasma and urine ketone concentrations and decreased serum bicarbonate concentration.5 When this does not occur, it should raise suspicion of dysregulated insulin secretion or disorders of fatty acid oxidation. Our findings may have been influenced by the inclusion of neonates in the study population, and in turn, the high proportion of children with previously undiagnosed hyperinsulinism. Neither the duration of illness nor decreased oral intake was associated with establishing a hypoglycaemia diagnosis. However, the high level of missingness for these variables potentially limits interpretation of these findings. Children in whom a diagnosis was established had lower weight-for-age, but weight status (weight adjusted for length/height) did not statistically significantly differ between groups. Absence of documented medical or surgical comorbidities at presentation also emerged as associated with establishing a diagnosis. Reasons for this finding are less obvious but may also stem from the inclusion of neonates.
While the patients with growth hormone deficiency and acute hepatic insufficiency had clinical features suggestive of the underlying aetiology of hypoglycaemia at presentation, the remainder did not. In fact, the child with hyperinsulinism in the setting of mosaic Turner syndrome, which is a recognised association,10 did not have classic phenotypic features of Turner syndrome. In this child’s case, a molecular diagnosis was incidentally uncovered during the genetic evaluation for hyperinsulinism.
A genetic diagnosis was suggested based on testing in 25% of patients in whom a hypoglycaemia disorder was identified. Overall, genetic testing yielded information supporting an underlying aetiology of hypoglycaemia in 11% of patients in whom it was obtained. In a prior study of children with ketotic hypoglycaemia and non-diagnostic metabolic and endocrine evaluation, genetic testing revealed mutations in genes involved in glycogen synthesis and degradation in 12%.11 Interestingly, no cases of glycogen storage disease were identified in our cohort though it is notable genetic evaluation was not universally performed.
Our findings need to be interpreted in light of several limitations. As a retrospective study, data was subject to potential inconsistencies or omissions in documentation in the EHR. Although diagnoses of hypoglycaemia were biochemically confirmed, it is likely that potential subjects were not identified because hypoglycaemia was not listed as a diagnosis or reason for consultation. Decisions to obtain an initial plasma glucose level, consult endocrinology and pursue diagnostic evaluation were each at the discretion of the provider. Selection bias could have resulted from differential decision-making at each of these levels. We explored potential sources of bias stemming from the latter of these by comparing those who did versus did not undergo a diagnostic fast; however, this analysis fails to capture the role of unmeasured factors driving differential selection of subjects. This was a single-centre study in which children were evaluated by endocrinologists with expertise in hypoglycaemia disorders at a large children’s hospital. Findings may not be generalisable to different populations, particularly those including children with different age distributions.
Despite these limitations, this study adds to the sparse body of literature examining the frequency of underlying pathology among children with hypoglycaemia during intercurrent illness. Our findings highlight the importance of obtaining a ‘critical sample’ or at a minimum, assays for bicarbonate and beta-hydroxybutyrate at the time of hypoglycaemia as these studies are both readily available and informative in differentiating between categories of hypoglycaemia disorders. This approach is in keeping with Pediatric Endocrine Society recommendations for evaluation of hypoglycaemia in children.5 Without appropriate evaluation, these children may not be identified, and consequently, appropriate treatment may not be implemented.
Conclusions
The high frequency of hypoglycaemic disorders identified in this study underscores the critical importance of investigating children with hypoglycaemia during illness and argues against ascribing findings to prolonged starvation. Endocrinology should be consulted to guide the diagnostic evaluation. Young age and absence of ketosis and acidosis at presentation were identified as potential predictors. These findings need to be confirmed in future studies.
Data availability statement
Data are available upon reasonable request. Data that support the findings of this study are included in this article and its online supplemental material file. Further enquiries can be directed to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study was determined to be exempt by the Children’s Hospital of Philadelphia Institutional Review Board. Patients were not involved in the design or conduct of this study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ER and OA are joint first authors.
Contributors OA and ER share first authorship. OA and ER codrafted the first version of the manuscript. OA performed electronic health record data extraction. ER conducted data analyses. DDDL conceptualised the work and edited the manuscript. DDDL is the guarantor of this work and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This work was supported by National Institute of Diabetes and Digestive and Kidney Diseases grant R01 DK056268 awarded to DDDL and by National Institute of Neurological Disorders and Stroke grant T32 NS091006 awarded to ER. The funding agencies did not have any role in study design, collection, analysis, interpretation of data, or writing of the report.
Competing interests DDDL has received research funding from Crinetics Pharmaceuticals, Twist Bioscience, Hanmi Pharmaceutical, Ultragenyx, Zealand Pharma and Rezolute for studies not included in this manuscript. DDDL has received consulting fees from Crinetics Pharmaceuticals, Zealand Pharma, Heptares, Eiger Biopharma, Hanmi Pharmaceutical, Poxel, Rezolute, Soleno Therapeutics, Slingshots Insights, and Triangle Insights, honorarium for lectures from Hasbro Children’s Hospital, Saudi Society of Endocrinology and Metabolism, University of Kentucky, University of Chicago, Joslin Research Center, Children’s Hospital of Helsinki, Nemours Children’s Health System, Chinese Society of Pediatric Endocrinology and Metabolism, and Massachusetts General Hospital, and travel support for conference presentations from Sociedad de neonatologia de Puebla, Sociedad ecuatoriana de pediatria, International Pediatric Association, Children’s Hospital of Helsinki, and Massachusetts General Hospital not related to this manuscript. DDDL is named as an inventor in USA Patent Number 9616108, 2017; USA Patent Number 9821031, 2017; Europe Patent Number EP 2120994, 2018; and Europe Patent Number EP2818181, 2019; which cover the use of exendin-(9-39) for treating hyperinsulinism and postprandial hypoglycaemia and has donated all financial proceeds from these patents to the Children’s Hospital of Philadelphia. DDDL participates on the advisory boards of Soleno Therapeutics and the NIH: RADIANT Study and on the Scientific Advisory Board of Congenital Hyperinsulinism International. DDDL has received donated research supplies from Dexcom for studies not included in this manuscript. DDDL holds stock options at Merck. ER and OA do not have any relevant disclosures to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.