Article Text

Abstract
Background Hyperbilirubinaemia is a silent cause of newborn disease and death worldwide. However, studies of the disease in sub-Saharan Africa are highly variable with respect to its prevalence. Hence, this study aimed to estimate the overall magnitude of neonatal hyperbilirubinaemia and its association with glucose-6-phosphate dehydrogenase (G6PD) deficiency and blood-type incompatibility in sub-Saharan Africa.
Methods PubMed, Scopus, Google Scholar and the Cochrane Review were systematically searched online to retrieve hyperbilirubinaemia-related articles. All observational studies reported the prevalence of hyperbilirubinaemia in sub-Saharan Africa were included for analysis and excluded if the study failed to determine the desired outcome. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed. Heterogeneity across the included studies was evaluated using the inconsistency index (I2). Subgroup and meta- regression analysis were also done. Publication bias was examined by funnel plot and the Egger’s regression test. The random-effect model was fitted to estimate the pooled prevalence of neonatal hyperbilirubinaemia. The meta-analysis was performed using the STATA V.14 software.
Results A total of 30 486 studies were collected from the different databases and 10 articles were included for the final analysis. The overall magnitude of neonatal hyperbilirubinaemia was 28.08% (95% CI20.23 to 35.94, I2=83.2) in sub-Saharan Africa. Neonates with G6PD deficiency (OR 2.42, 95% CI 1.64 to 3.56, I2=37%) and neonates that had a blood type that was incompatible with their mother’s (OR 3.3, (95% CI 1.96 to 5.72, I2=84%) were more likely to develop hyperbilirubinaemia.
Conclusion The failure to prevent and screen G6PD deficiency and blood-type incompatibility with their mother’s results in high burden of neonatal hyperbilirubinaemia in sub-Saharan Africa. Therefore, early identification and care strategies should be developed to the affected neonates with G6PD deficiency and blood-type incompatibility with their mother’s to address long-term medical and scholastic damages among those exposed to hyperbilirubinaemia
- statistics
- qualitative research
- nursing Care
- jaundice
- neonatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Neonatal hyperbilirubinaemia is a common cause of neonatal morbidity and mortality, particularly in low-income nations.
The reported prevalence of neonatal hyperbilirubinaemia in sub-Saharan Africa is inconsistent.
What this study adds?
The overall magnitude of neonatal hyperbilirubinaemia was estimated to be 28.08% (95% CI 20.23% to 35.94%) in sub-Saharan Africa.
Neonates with glucose-6-phosphate dehydrogenase deficiency and neonates that had a blood type that was incompatible with their mothers’ were more likely to develop hyperbilirubinaemia.
Background
Neonatal hyperbilirubinaemia (ie, jaundice) is a common and often a benign condition that afflicts many infants in the first week of life. It is caused by the accumulation of bilirubin in the skin, which is created from biliverdin, a breakdown product of heme. Over 50% of newborns get jaundice in the first few days of life, and from those, 60%–80% leads to unpreventable condition in newborns worldwide.1 Elevated levels of conjugated bilirubin (ie, conjugated bilirubin level being ≥20% of the total serum bilirubin) are always pathologic and occur due to intrahepatic or extrahepatic obstruction of the biliary tract. Moreover, elevated levels of unconjugated bilirubin is the most common reason for neurological sequelae related to hyperbilirubinaemia.2 The most significant among the long-term complications of hyperbilirubinaemia is kernicterus, which is a type of brain damage that leads to choreoathetosis, sensorineural hearing loss, dental enamel dysplasia, paralysis of upward gaze, hypotonia and a delay in the acquisition of motor skills, with a significant risk of neonatal death.3
The prevalence of hyperbilirubinaemia in the neonates of sub-Saharan Africa is somewhat inconsistent in the current literature, with rates ranging from 4% to 45.8%.4–7 That said, the burden of this condition on medical systems in developed and developing nations is significant.1 There are many risk factors that can predispose infants to hyperbilirubinaemia, including jaundice observed in the first 24 hours, blood group incompatibility, other known haemolytic disease, elevated end-tidal carbon dioxide, gestational age of 35–36 weeks, sibling received phototherapy, cephalohematoma, significant bruising, excessive weight loss, isoimmune haemolytic disease, glucose-6-phosphate dehydrogenase (G6PD) deficiency, asphyxia, temperature instability, sepsis, acidosis and albumin <3 g/dL.2 7 8 More than any other risk factors, G6PD deficiency and blood group incompatibility are the most significant contributing causes for neurotoxicity.2 More than 70% of hyperbilirubinaemia cases are due to either idiopathic neonatal hepatitis or biliary atresia.3
Although G6PD deficiency and blood group incompatibility are widely regarded as risk factors for hyperbilirubinaemia, the literature does show some inconsistencies.7–14 For instance, several studies from sub-Saharan African countries7 9–11 have indicated that G6PD deficiency and blood incompatibility are associated with an increased risk of neonatal jaundice. However, another study showed that they were not associated with jaundice.12 Given this variability and the lack of pooled representative data, we aimed to estimate the pooled burden of neonatal hyperbilirubinaemia in countries of sub-Saharan Africa. Moreover, we attempted to identify its association with G6PD deficiency and blood-type incompatibility in this region. These data will aid healthcare professionals in assessing the prevalence of hyperbilirubinaemia in their population and hopefully allow them to properly allocate resources to combat this neonatal affliction.
Methods
Data sources and literature search strategy
This systematic review and meta-analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Pertinent published articles were searched independently and systematically by the authors in the following electronic databases: PubMed, Google Scholar, African Journals Online, Scopus and others (Grey literature, such as unpublished articles and conference abstracts). In addition, a manual search of grey literature was performed to find other significant studies. The searches were limited to full text, open access articles with human subjects that were written in any language. Authors were contacted for full texts of their articles through email, if necessary. The search was conducted using the following terms and phrases: “magnitude neonatal hyperbilirubinemia,” “neonatal jaundice,” “glucose-6-phosphate dehydrogenase deficiency,” “blood type incompatibility” and“sub-Saharan Africa”. Boolean operators like “and” and “or” were used to combine search terms. Particularly, to fit the advanced PubMed database, the following search strategy was used: (“magnitude neonatal hyperbilirubinemia” OR “glucose-6-phosphate dehydrogenase deficiency” OR “blood type incompatibility”) AND (“sub-Saharan Africa”).
Eligibility criteria
Predefined inclusion criteria
Studies were included for further analysis if they conformed to the following criteria: (1) All observational studies reported the prevalence of hyperbilirubinaemia (2) the study setting was somewhere in sub-Saharan Africa (3) the study participants were newborns with severe hyperbilirubinaemia (4) publication condition: all published and unpublished articles (5) All languages were included (6) Publication date: Until 10 April, 2020, and (6) the article was an observational study, and a retrospective or prospective cohort study or a cross-sectional study
Exclusion criteria
Studies were excluded from this systematic review and meta-analysis if they fulfilled one of the following: (1) we were unable to access the full-text articles after two emails to the principal investigator (2) a study was a duplicate of a previously identified study (3) the study did not fulfil the inclusion criteria and (4) failed to determine the desired outcome.
Type of exposure
In this meta-analysis, G6PD deficiency and blood-type incompatibility were considered the exposure variables to estimate their effects on neonatal hyperbilirubinaemia.
Outcome of interest
Prevalence of neonatal hyperbilirubinaemia (conjugated/unconjugated).
Methods for data extraction and quality assessment
We used a Microsoft Excel standardised data extraction form to extract the data. The following information was extracted from each incorporated study: the name of the first author, publication year, country name, study design, total sample size, final included sample size’, response rate, study settings and OR with 95% CI. The number of children with neonatal hyperbilirubinaemia was also extracted from the studies and prevalence was calculated using the final included sample size. Data extraction from source documents was done independently by all investigators. Disagreements were resolved by consensus. The quality of the included studies was evaluated by using the Newcastle-Ottawa Scale (NOS).13 Specifically, NOS assessed the sample representativeness and size, the comparability between participants, how neonatal hyperbilirubinaemia was ascertained and the statistical quality of each study. Studies were included for further analysis if they scored ≥5 out of 10 points in three domains of ten modified NOS components.
Data processing and analysis
Data were extracted from Microsoft Excel and analysed using STATA V.14 statistical software and forest plots that showed combined estimates with a 95% CI. The overall pooled prevalence was estimated by random effect meta-analysis.14 Heterogeneity was assessed by computing p values for the inconsistency index (I2).15 We found significant heterogeneity among the studies (I2=83.2%, p=0.001). Meta-regression analysis was performed using sample size, study design and country, factors and publication year to explore the possible source of heterogeneity. We also conducted a subgroup analysis using the following variables: study design, publication year, sample size, study design and locations of the studies. Sensitivity analysis was also conducted to assess the possible included outlier articles publication bias was assessed using a funnel plot and the Egger’s regression test.14 The association between the prevalence of neonatal hyperbilirubinaemia and G6PD deficiency or blood-type incompatibility was measured by random-effects meta-analysis pooled ORs.
Results
Search process
A total of 30 486 studies were collected from the aforementioned databases. After removing duplicates (n=29 927), a total of 559 studies were retrieved. Of which, 486 were rejected just by reading the titles of the articles (due to unrelated to the topic). Of the remaining 73 studies, 31 were excluded by abstracts (due to no abstract, unrelated abstracts and unable to access the full text of articles with two email contact). Full-text copies of the remaining 42 studies that potentially met the inclusion criteria were assessed. From this, 32 articles were discarded due to failed to determine the desired outcome (not fully fulfilled the inclusion criteria). After further screening, 10 papers were fulfilled the eligibility criteria for estimating the pooled prevalence and there are an additional two studies (Woimo (et al and Farouk et al) which do not provide prevalence data but do contribute to the analysis of the association between G6PD deficiency and neonatal hyperbilirubinaemia. Articles published in several languages were assessed. But, nine papers published in English and one paper published in French was retained for final analysis (figure 1).

Flow chart of how research articles were searched and selected for analysis in this study.
Characteristics of included studies
The pooled prevalence of neonatal hyperbilirubinaemia in sub-Saharan Africa was assessed using 10 studies involving a total of 12 327 participants. The minimum sample size was 91 participants in a study conducted at Awolowo University, Nigeria,16 while the largest sample size was also participants from Nigeria (5229).11 All studies involved populations from sub-Saharan Africa, with six involving participants from Nigeria,6 8 10 11 16 17 two from Ethiopia7 9 and one each from Zimbabwe,5 and Congo4 (table 1).Regarding the sampling technique employed, six of the studies7–9 16–18 used consecutive sampling to select study participants. However, the other studies did not report their sampling methods.
Baseline characteristics of the studies used to assess the pooled prevalence of neonatal hyperbilirubinaemia in sub-Saharan Africa
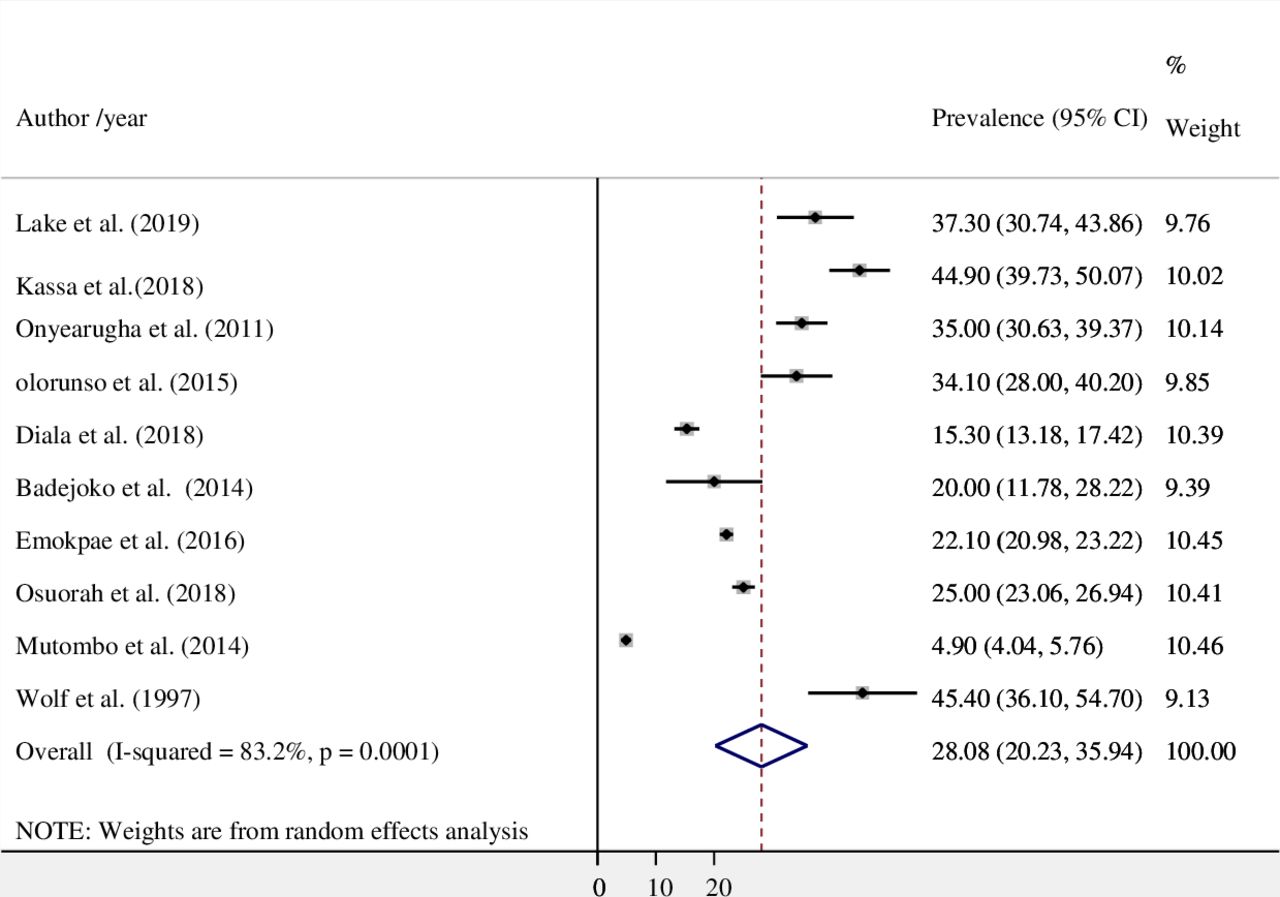
Magnitude of neonatal hyperbilirubinaemia
A total of 12 327 participants and 10 studies were included to estimate the pooled magnitude of neonatal hyperbilirubinaemia. The overall random effects estimate for the level of neonatal hyperbilirubinaemia across sub-Saharan Africa was 28.08% (95% CI 20.23 to 35.94) (figure 2). Our test statistics indicated a high level of heterogeneity (I2=83.2%) and the Eggers’ test showed no significant publication bias (p=0.36).

Magnitude of neonatal hyperbilirubinaemia in sub-Saharan Africa.
Subgroup analysis
We performed a subgroup analysis using sample size, publication year, study design and the location of the included studies. In the current meta-analysis a sample size of less than 384 revealed a higher prevalence(40.2, 95% CI 34.5 to 45.8, (I2=66%) as compared with sample size of greater than or equal to than 384 (20.3, 95% CI 11.3 to 29.4, I2=88). Our subgroup analysis based on study location also showed that the highest pooled prevalence was observed from studies done in Ethiopia (41.4%; 95% CI: 33.9 to 48.8, I2=68.6), . Prevalence rates were very similar across study designs (table 2).
Subgroup analysis results of the included studies
Meta-regression analysis
To identify the sources of heterogeneity in this study, meta-regression analysis was performed by considering the sample size, study design and country, factors and publication year. However, our results showed that those covariates were not significantly associated with the presence of heterogeneity (table 3).
Meta-regression results by different covariant
Publication bias and quality status
Publication bias was evaluated by a funnel plot and the Egger’s regression test. With respect to the former, publication bias is represented as significant asymmetry in a funnel plot. As depicted in figure 3, there was a significant amount of symmetry in our funnel plot and thus there was publication bias. The Egger’s regression test confirmed this result with a p=0.36. The quality assessment for each study is shown in online supplemental file 2.
Supplemental material

Funnel plot to determine publication bias among the included studies.
The association between G6PD deficiency and neonatal hyperbilirubinaemia
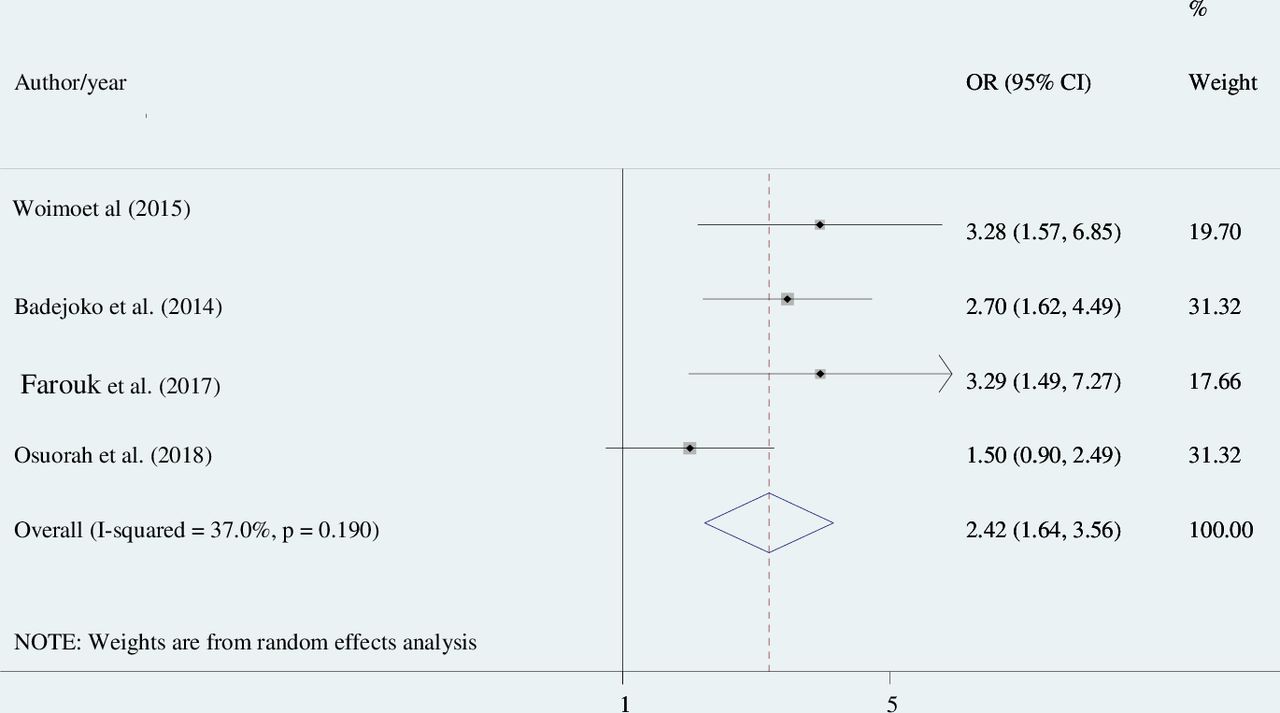
The association between neonatal hyperbilirubinaemia and G6PD deficiency was reported in four articles,6 16 19 with a total of 3353 neonates. The pooled OR from these studies was 2.42 (95% CI 1.64 to 3.56, I2=37.0%, p=0.19), indicating that the likelihood of hyperbilirubinaemia was 2.42 times higher in neonates with a G6PD deficiency than those with normal G6PD levels (figure 4).

The association between G6PD deficiency and neonatal hyperbilirubinaemia in studies from sub-Saharan Africa. G6PD, glucose-6-phosphate dehydrogenase.
The association between blood type incompatibility and neonatal hyperbilirubinaemia
Blood-type incompatibility was another contributing factor for neonatal hyperbilirubinaemia and their connection was reported in five studies included in our analyses6 7 9–11 by involving a total of 8820 participants. The pooled OR was 3.3 (95% CI 1.96 to 5.72, I2=84.0%, p=0.0), suggesting that the risk of developing hyperbilirubinaemia was 3.3 times higher among neonates with an incompatible blood type as compared with blood-type compatible infants (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The association between blood-type incompatibility and neonatal hyperbilirubinaemia in studies involving sub-Saharan African populations.
Discussion
Neonatal hyperbilirubinaemia remains the principal reason of morbidity and mortality in resource-limited nations.4–7 The prevalence is also variable across different studies.4–7 Inconsistence estimates are reported in the association with G6PD deficiency2 7 8 and blood-type incompatibility.2 7 8 So that, this meta-analysis determined the pooled prevalence of neonatal hyperbilirubinaemia and its association with G6PD deficiency and blood type incompatibility in sub-Saharan Africa using 10 studies. The overall pooled estimate for the prevalence of hyperbilirubinaemia was 28.08% (95% CI 20.23 to 35.94). This is consistent with the rates of neonatal hyperbilirubinaemia in the USA.20 However, our finding is higher than that found in a previous meta-analysis.21 In contrast, the prevalence of hyperbilirubinaemia found in our study was substantially lower than that found in previous systematic reviews carried out in Pakistan,22 Myanmar23 and global burden diseases GBD.24 25 These differences might be the result of different diagnostic standards for neonatal hyperbilirubinaemia, early diagnosis and treatment in developed countries, and the early discharge of healthy late-preterm and full-term newborns.
The prevalence of neonatal hyperbilirubinaemia varied greatly in the included studies, ranging from 4.9%4 to 44.9%.9 However, our subgroup analysis based on study location showed that the highest pooled prevalence was observed from studies done in Ethiopia (41.4%; 95% CI 33.9 to 48.8). This variation could be attributed to the differences in healthcare facilities. With emerging of an inexpensive technology, the developed nation’s strategy for prevention and treatment of neonatal hyperbilirubinaemia can more feasibly reach those at risk in resources-limited settings. Additionally, a screening strategy of postnatal haemolysis and management of idiopathic aetiologies may help eradicate mortality and morbidity-related jaundice.
In this study, the odds of an infant getting hyperbilirubinaemia was 2.4 times higher for those neonates with a G6PD deficiency than those with normal G6PD levels. This is in line with studies done in different countries.18 23 26–28 G6PD deficiency may be linked to hyperbilirubinaemia because G6PD is the main source for Nicotinamide adenine dinucleotide phosphate(NADPH) in red blood cells, which is important for antioxidant defence. Those neonates that are deficient in G6PD are susceptible to oxidant-induced haemolysis and hemecatabolism that produces bilirubin—the precipitating factor in hyperbilirubinaemia.29
This study also noted that the likelihood of having hyperbilirubinaemia was higher among neonates with blood group incompatibility. Neonates with blood group incompatibility were 3.3 times more likely to have hyperbilirubinaemia as compared with patients with a compatible blood type. This is supported by a number of previous studies.23 30 This could be due to haemolysis that occurs when maternal immunoglobulin G anti-A or anti-B antibodies cross the placenta and attach to the opposite antigen site on the neonatal red cell,which results in increase heme catabolism that increases the production bilirubin.31
The implication of the current finding is stated as follows; estimating the prevalence of neonatal hyperbilirubinaemia and its association with G6PD deficiency and blood-type incompatibility will help to mobilise the national leadership to initiate actions and embed proven systems, policies and programmes to reduce jaundice-related newborn mortality and disabilities. It will also help to the healthcare professionals to include neonates born with G6PD deficiency and blood-type incompatibility as Every Newborn Action Plan promotion of maternal and newborn care and essential newborn care for better care of neonates with jaundice which helps better neonatal survival, improved long-term development and decrease disability. Moreover, the fading will also alarm them for national identification of all blood type incompatible woman before or during pregnancy and with coordinated obstetric and neonatal care.
Strengths and limitations of the study
As far as we know this is the first meta-analysis which has been done in sub-Saharan Africa. This study was conducted with the use of an inclusive search strategy to incorporate the studies involving African patients. All of the included studies had high methodological quality based on our NOS assessments. Despite this, our study had several limitations. First, most of the studies used for this analysis had a small sample size, which could have a significant effect on the estimated prevalence of neonatal hyperbilirubinaemia. Moreover, this meta-analysis represented only studies from five countries, which may be an under-representation for the region of sub-Saharan Africa.
Conclusion
The prevalence of hyperbilirubinaemia in sub-Saharan Africa is quite high and a major percent of this is due to G6PD deficiency and blood group incompatibility. Based on our findings, we suggest that all neonates with hyperbilirubinaemia be assessed for G6PD deficiency and blood-type compatibility. Additionally, incorporating the G6PD screen as a newborn screening programme can be a cost-effective strategy to deal with this problem. Assessing ABO incompatibility following discharge, bilirubin estimation and plot on normogram, and follow the babies as per the risk stratification would be the best strategy. Furthermore, additional research is needed to identify other associated factors for the development of neonatal hyperbilirubinaemia.
Supplemental material
Acknowledgments
We would like to thank to Doctor Ryan Bell (CEO and Chief Editor Excision Editing) whose assistance was invaluable to the completion of the study and who have made an extensive edition in our manuscript.
References
Footnotes
Contributors YAA conceived and designed the study. YAA and WSS established the search strategy. WSS, TYA and GBM wrote the review. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information. The data analysed during the current meta-analysis is available from the corresponding author on reasonable request.