Article Text

Statistics from Altmetric.com
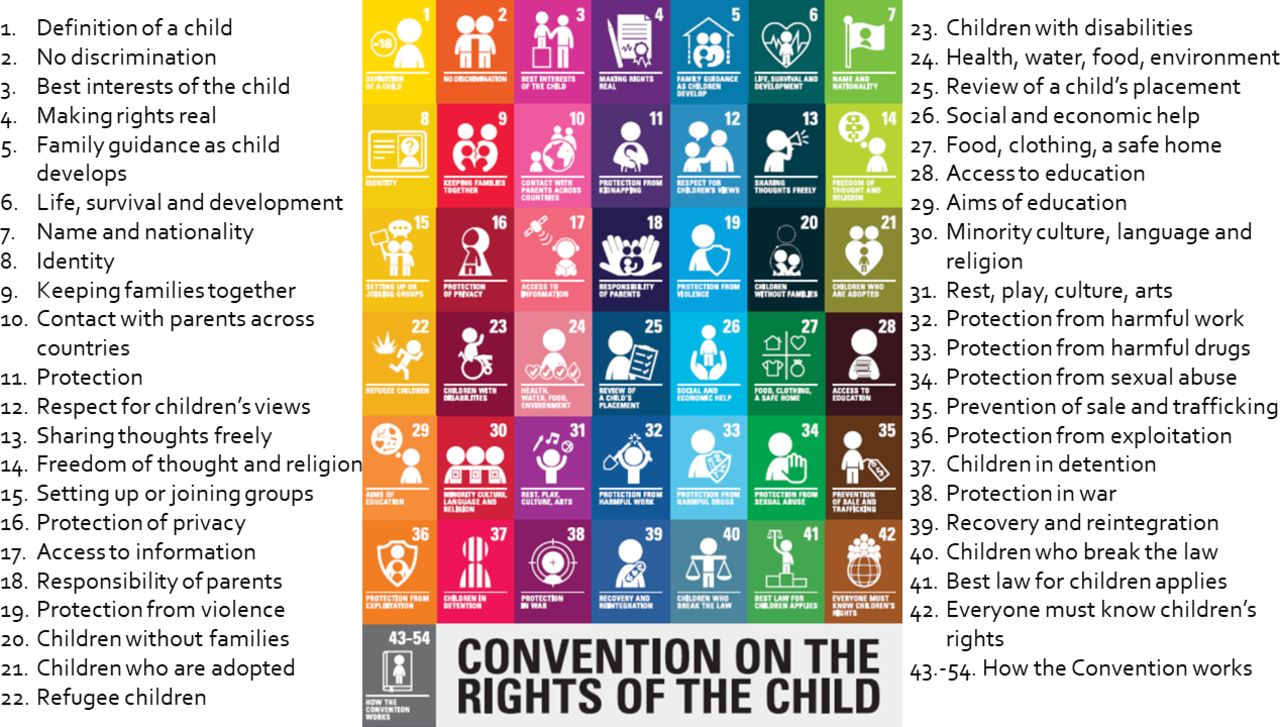
With the launch of the United Nations (UN) Convention on the Rights of the Child (CRC) in 19891 (figure 1), world leaders embraced an aspirational vision for childhood and the health and well-being of children. Over the ensuing decades, every UN member nation except the USA has ratified the CRC. The Sustainable Development Goals (SDGs),2 which include a substantial focus on children, have further solidified the global commitment to advance the rights of children to life and optimal survival and development (CRC, Article 6).

{kind=link}
United Nations (UN) Convention on the Rights of the Child.
A taxonomy of the articles of the UN Convention on the Rights of the Child
The 40 substantive rights articulated in the CRC provide a blueprint for optimising the health and well-being of children. The failure of the USA to ratify the CRC and implement a child rights-based approach (CRBA) to child health3 has contributed to poor health outcomes for American children in comparison to other high-income countries (HICs). By not recognising children’s rights to optimal survival and development (CRC, Article 6) and health and healthcare (CRC, Article 24), large numbers of children continue to be deprived of the resources and services they require to optimise their health and well-being. Similarly, by not addressing promotion and protection rights of children related to the social determinants of health, the basic needs of children remain unfulfilled resulting in gross child health and social inequities. As documented by the UNICEF Innocenti Centre in 2013, the USA ranked 26th among 29 HICs for overall child well-being.4 In 2020, the USA slid to 32nd and 38th among 38 HICs for mental and physical well-being.5
A CRBA, grounded in the rights articulated in the CRC, would provide a strategy for contextualising and responding to the multiple challenges confronting children in the USA. From a legal perspective, ratification of the CRC would establish the USA’s obligation and accountability to address the holistic needs and rights of all children—including providing the highest quality of education, health and disability services; protection from exploitation, violence, family separation and bias in the juvenile justice system; and ensuring their rights to participation in all aspects of their lives. The USA also fares poorly in these domains in comparison to other HICs.
The 40 substantive rights in the CRC and the 17 SDGs also provide the metrics and a methodology required to monitor communities’ progress in fulfilling children’s rights.6 Further, a CRBA would expand the capacity to respond to the social determinants of health by addressing the CRC articles related to children’s civil-political, social, economic and cultural rights (table 1). Though the USA was actively engaged in drafting the CRC, there are multiple reasons why it has failed to ratify it. These barriers, detailed in table 2, include those dealing with US sovereignty and federalism, legal issues, politics and parental rights.
Reasons why the USA has failed to ratify the UN Convention on the Rights of the Child
In addition to the articles themselves, adoption of the human rights principle of the Interdependence of rights would help ensure the needs of the whole child are considered in efforts to achieve optimal health and well-being. Similarly, adoption of the principle of Universality would help minimise the widespread discrimination in the USA against children based on race, ethnicity, sexual orientation, and immigration and socioeconomic status—and advance health parity among states. A CRBA would additionally provide US child health professionals with tools and a parlance for child advocacy, and mobilise and amplify the voice of children.
However, there is now an even more pressing need for the USA to embrace the principles, standards, norms and parlance of human rights—as a national and global response to the rise of authoritarian regimes and threats to democracies—a rise and fall that has been well documented over the past decade.7
Where along the continuum of populism to authoritarianism and fascism countries throughout the world have devolved is a question for political scientists to debate. However, regardless of where they fall on this continuum, the practice of targeting minority groups is foundational to their devolution. In Nazi, Germany, it was the Jews, among others. Today in India, it is Muslims. In Hungary, it is immigrants and lesbian, gay, bisexual and transgender people. In Myanmar, it is Rohingyas. In China, the Uighurs. In Brazil, indigenous populations. And in the USA, among the many minority and immigrant groups that are targeted, children and youth are being used as political pawns to support the rise of illiberal politics.
The use of children as political tools has a long history in the USA with lasting consequences. For example, the myth of minority youth super predators in the 1980s served as a catalyst for the disproportionate incarceration and involvement of Black youth in juvenile justice systems, which has decimated the lives and futures of generations of minority children.8 These myths have served as a pretext for advancing racist policies that continue to nurture far right-wing politics throughout the USA.
Now, decades later, the conservative movement is pursuing new strategies that exploit children—with grave consequences. Over the past 2 years, politically motivated public health policies have been implemented throughout the USA in response to the COVID-19 pandemic to ban masks and evidence-based quarantine practices in schools, and undermine vaccination of children against COVID-19 and other childhood illnesses. Policies have been implemented targeting lesbian, gay, bisexual, transgender and queer (LGBTQ) youth, including ending healthcare coverage for trans-specific care for children, prohibiting education about LGBTQ persons in schools, removing support for LGBTQ students in classrooms that previously served as safe havens and eliminating the confidentiality of student–teacher/counsellor conversations. Among the hundreds of recent anti-transgender legislative initiatives pursued in the USA, the majority have focused on children and youth.9
Education and discussion about racism and racial identity are now being curtailed throughout the country. In Florida, curricula have been rewritten to erase these issues, teachers are forbidden to address them and books that mention them are being banned from school libraries, as they are in many other states. Throughout the USA, courts and school boards previously considered non-partisan have become the arena for partisan assaults on children. These policies are spawning groups who use ‘parental rights’ as a fulcrum to violate and eliminate children’s rights in their pursuit of political power. The Florida Parental Rights legislation, passed in 2021, provides insights into these political strategies.
A response in the USA, grounded in the principles and parlance of child rights, will be necessary to help thwart the advance of authoritarianism—in the USA and abroad. The history of the medical profession’s complicity and failure to actively counter the rise of repressive regimes, including collaboration of the medical profession with the Nazis,10 is relevant and instructive to what is unfolding in the USA and other countries. The use of children and youth as political pawns in the USA demands the vociferous voice and courageous action of paediatricians, organised medicine and all child health professionals to advance the rights of children as a bulwark against the rise of authoritarianism. Ratification of the CRC is critically important in this regard.
While the USA remains the sole country that has failed to ratify the CRC, global gaps remain between the vision for and realities of the global health and well-being of children and childhood. In many respects, these gaps reflect the chasm between child rights as aspirational and their translation into practice—gaps that are increasingly strained by global challenges—including the rise of illiberal regimes. To be sure, global progress in the realisation of children’s rights has occurred, but these gains remain fragile and tenuous.
Ratification of the CRC by the USA, coupled with the implementation of a CRBA to the global challenges affecting children, including climate change, globalisation, environmental injustice, armed conflicts, forced migration, the rise of populist autocracies, income inequities and the SARS-CoV-2 pandemic, would help advance the realisation of the rights of children throughout the world to life and optimal survival and development. Without such rights-based policies and strategies, the USA cannot address the needs of its children, nor play a leadership role in addressing the increasingly complex challenges of children worldwide.
Unfortunately, US ratification of the CRC is unlikely to occur in the foreseeable future. Efforts by multiple organisations, including the American Academy of Pediatrics and the Campaign for the US Ratification of the UN Convention on the Rights of the Child, have all failed, and have been suspended. Since the Clinton administration signed the CRC in 1995, no Democratic or Republican president has submitted the CRC to the Senate for ratification.
However, the foundational principles, standards and norms of child rights and the framework provided by the CRC are as relevant to the USA as they are to other countries. Though important, time and energy spent on ratifying the CRC may now be better expended on implementing and demonstrating the value of a CRBA to the health and well-being of children. The first step in this journey is fulfilling CRC Article 42: ‘States Parties undertake to make the principles and provision of the Convention widely known, by appropriate and active means, to adults and children alike’. Progress is being made in this regard. Important national gains are being made in mobilising the voice of youth. A Child Friendly Cities movement is expanding across the country, supported by the US Committee for UNICEF. The parlance of child rights is beginning to permeate professional paediatric organisations, meetings and publications. Foundations are now beginning to understand the relevance of child rights to achieving their missions.
Though the USA is a world leader in child health research, and expends substantial resources on child healthcare, it lags far behind other HICs with respect to child health outcomes.5 The USA, for multiple historical, political and cultural reasons, is blind to the needs and rights of children. Given the status and inequities in child health in the USA, and the political realities we face, we must prioritize the implementation of the principles, standards and norms of child rights as a strategy to improve child health and well-being, and as a bulwark against the political undertow that is dragging the USA and other countries into the depths of fascism.
Ethics statements
Patient consent for publication
Footnotes
Twitter @doctorlix
Contributors All authors performed literature searches and were equal in the planning, conception and design, acquisition of data or analysis and interpretation of data, and the conduct and reporting of the work in this paper. All authors have seen and approved the final version of the manuscript, figures, tables and references for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.