Article Text

Abstract
Background Childhood vitiligo differs from adult vitiligo in many aspects. To the best of the authors’ knowledge, there is no systematic review of different clinicoepidemiological patterns of vitiligo in children. This study aimed to review the characteristics of vitiligo among the paediatric population.
Methods In June 2022, a comprehensive search was conducted using MeSh-based keywords on online databases including PubMed, Scopus and Web of Sciences. The papers were assessed, and the eligible articles were selected. The selection of articles followed three distinct steps. The extracted clinicoepidemiological data were then imported into the STATA software for meta-analysis.
Results The meta-analysis of 17 studies with 4365 subjects yielded 2475 women (estimated=56.8%, 95% CI 54.45 to 59.22). The female-to-male ratio was determined to be 1.3:1. Meta-regression demonstrated a significant relationship between continents and gender (p=0.03). The most prevalent types of non-segmental vitiligo were vulgaris (42.49%), focal (27.21%) and acrofacial (17.8%). The pooled ratio of non-segmental to segmental was 4.6:1. The highest and lowest ratios were found in Africa with one study (estimated=11.56%, 95% CI −0.98 to 24.10) and America with two studies (estimated=3.02%, 95% CI 1.54 to 4.50), respectively. Using meta-regression, the relationship between continents and vitiligo type was found to be insignificant (p=0.47). Positive family history was recorded in 657 patients (estimated = 16.88%, 95% CI 13.37 to 20.39). Positive family history varied by country of study from 13.91% (Asia with 11 studies) to 27.01% (Europe with two studies) (p=0.11). Kobner phenomena and leukotrichia were noted in 687 (25.47%) and 461 (18.52%) patients, respectively.
Conclusion The review indicated that childhood vitiligo is more prevalent in women. Non-segmental forms of childhood vitiligo were the most common, including vulgaris, focal and acrofacial. The clinicoepidemiological pattern of childhood vitiligo is variable in different geographic areas.
- epidemiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Vitiligo is a life-altering condition. Childhood vitiligo differs from adult vitiligo in many aspects.
WHAT THIS STUDY ADDS
Vitiligo was most prevalent in Africa and more common in girls. The most frequent non-segmental vitiligo types were vulgaris (42.49%), focal (27.21%) and acrofacial (17.8%).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Awareness of the typical pattern of childhood vitiligo in different geographic areas and its associated factors worldwide improves clinical disease identification and management.
Introduction
Vitiligo, an acquired autoimmune inflammatory disease of the skin, is a life-altering condition. The disease is primarily associated with significant cosmetic reports and significant psychological effects, including the social stigma that lowers affected individuals’ self-esteem.1
Childhood vitiligo is different from adult vitiligo in many aspects,2 where negative experiences from childhood vitiligo may influence adult life.3 Recent studies in the USA showed that 1.9 million cases had been diagnosed with vitiligo, and its prevalence is 0.76%.4 However, its prevalence varies from 0.5% to 2% in other countries.5 The exact prevalence of vitiligo in children is unknown, but at least 25% of cases begin before the age of 10.6 Although vitiligo with a very early onset has been reported, the existence of true ‘congenital vitiligo’ remains controversial.7
The precise mechanism underlying vitiligo is not fully understood. Autoimmune, neurogenic and self-destructive mechanisms are among the hypotheses reported.8 Exposure to environmental triggers such as trauma and sun exposure also have a significant role in vitiligo pathogenesis.9 Some studies also reported its association with other autoimmune diseases, including hypothyroidism, diabetes mellitus, alopecia, anaemia, lupus, rheumatoid arthritis and psoriasis. In addition, this disease is more prevalent among people with a positive family history of vitiligo.10
Several characteristics distinguish childhood vitiligo from adult vitiligo, including a higher prevalence of segmental variant, a higher prevalence of halo nevi and a higher prevalence of a family history of autoimmune diseases. All races can be affected by childhood vitiligo, but the prevalence and pattern of the disease likely vary by geographic origin.
Understanding the clinicoepidemiologic characteristics of vitiligo in the paediatric population appears to correlate with positive treatment outcomes.7 Clinicoepidemiologic characteristics of paediatric vitiligo were described in several epidemiological studies. However, no comprehensive review exists in this regard. This study aimed to review the characteristics of vitiligo among the paediatric population through a systematic review and meta-analysis.
Methods
Literature search strategy
The present study is a systematic review and meta-analysis to evaluate the clinicoepidemiological features of vitiligo in children. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was considered for this study. After consulting with experts in the fields of dermatology and paediatric dermatology, the MeSh databases were used to select keywords. The search was conducted on June 2022, where PubMed, Scopus and Web of Sciences were searched. All databases were searched using the following queries limited to the title: ((vitiligo) AND (epidemiology OR Clinical OR characteristics)) AND (Child OR Pediatric OR Children OR Infants OR Neonate)). In addition, an exploratory, non-systematic Google search was conducted to locate any missed articles and grey literature.
Inclusion and exclusion criteria
Studies were eligible if they met all of the following inclusion criteria: (a) they were observational epidemiological studies; (b) they included patients with vitiligo under the age of 18. Conference articles, abstracts, protocols, narrative and systematic reviews, consensus opinions and articles published in non-English languages were excluded from the study. No time limitation also was considered.
The records were imported into EndNote V.X8 software (V.8.0.1. Clarivate Analytics). The duplicated results were removed through the EndNote software function.
Study selection and appraisal
Included articles were screened through three steps. Initially, the authors screened the title of the articles and unsuitable and irrelevant articles were excluded. Second, the authors studied the abstract of the remaining articles, and irrelevant records also were excluded. Finally, the authors attempted to retrieve the full texts of the articles. All processes were completed independently by the authors to diminish the risk of bias. Two researchers independently screened the studies by title and abstract to identify articles that appeared to be relevant for a second screening. Following this, two researchers independently examined the complete texts of the remaining papers and identified studies that met the inclusion and exclusion criteria for the review. Disagreements between the two researchers were resolved through discussion. A third author reviewed the study and made the final decision if disagreements persisted. To improve the quality of the review, the journal and author names were concealed using a blind method.
Data extraction
The extracted data from each study included the name of the first author, the year of the study, the country of the study population, the number of the study population, age, gender, type of vitiligo, age of onset of vitiligo, systemic and cutaneous association, disease duration and family history of vitiligo.
Data analysis
STATA V.14 was used to perform the analysis through the ‘metan’ command. Begg’s funnel plot was employed to assess publication bias based on patient age, family history and type of vitiligo (segmental vs non-segmental). In addition, Begg’s and Egger’s tests were applied. Heterogeneity was assessed using the I2 index, and the random-effects method was employed to conduct the meta-analysis of its results. Forrest plots were drawn for variables of interest, including age and gender. Subgroup analysis was conducted only for a specific location (continent), and meta-regression was performed to determine the probable effect of time (year) and location (continent) on heterogeneity.
Patient and public involvement
Patients and/or the public were not involved in this research’s design, conduct, reporting or dissemination plans.
Results
Study characteristics
In this systematic review, 106 articles were identified after searching PubMed (25 articles), Scopus (49 articles) and Web of Sciences (32 articles). The duplicated records were then removed via EndNote software, and 41 articles remained. After screening the titles, five irrelevant titles were omitted, leaving 36 articles. Then, the authors evaluated the abstracts, and six articles with irrelevant abstracts were removed. In the final step, the full texts of remained articles were gathered and evaluated independently by the authors. Finally, 12 articles remained for final analysis. As previously mentioned, a Google Explorer search was also performed, and five new articles were added. Consequently, 17 articles were included in the final analysis. The PRISMA flowchart of the current study is shown in figure 1. As mentioned in the method, non-English articles were excluded by using the language filter tool. There were five non-English articles, three of them were in Portuguese language, one was in French language and one of them was in the Turkish language.
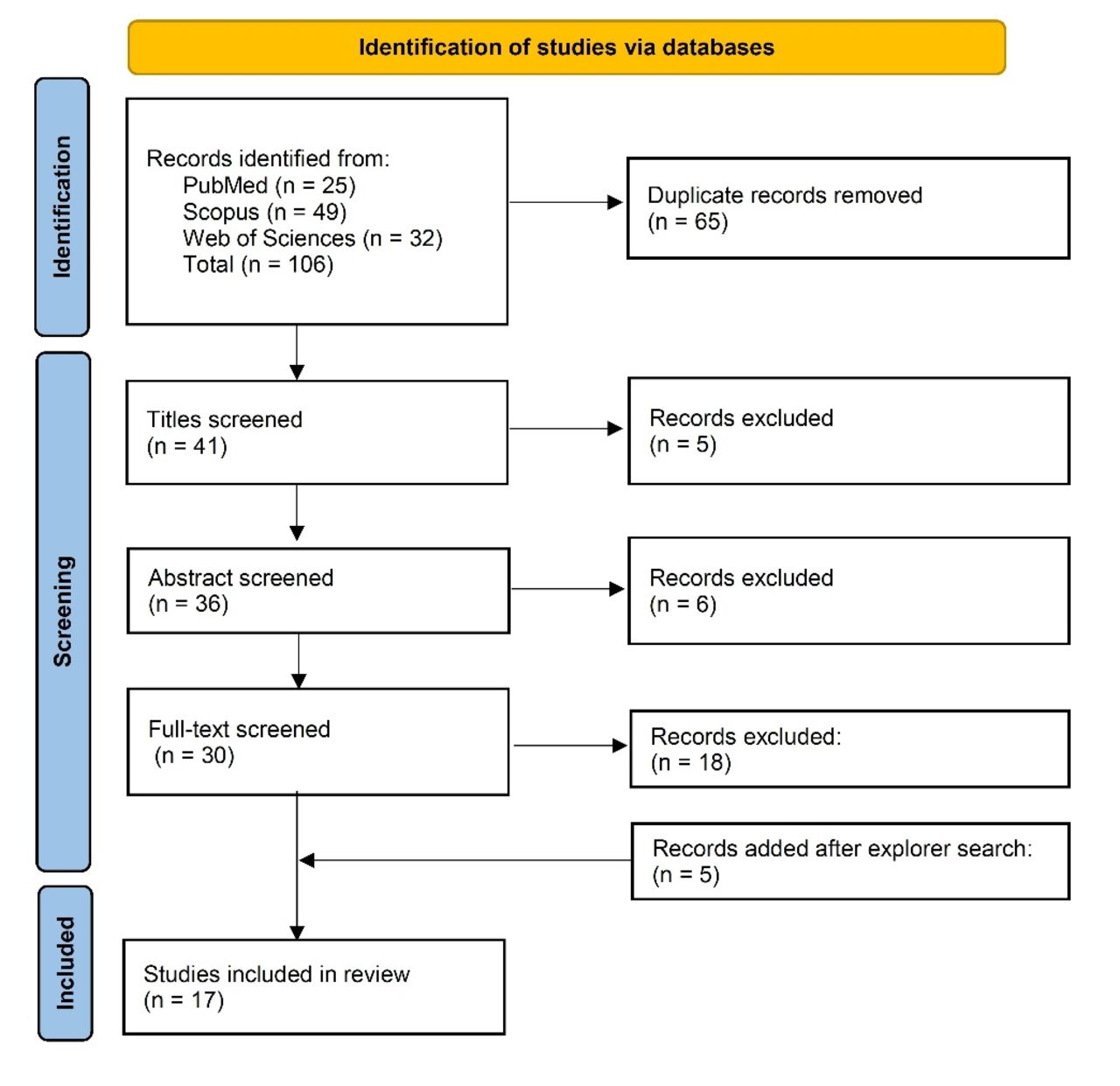
The PRISMA chart of the study. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The authors thoroughly reviewed these 17 articles, and the risk of bias was assessed using the National Institutes of Health-quality assessment tool. The outcome of the risk of bias assessment is shown in online supplemental file 1.
Supplemental material
The details of each study, including the author’s name, year of publishing, country, sample size, age, gender, type of vitiligo and family history, are summarised in table 1. Concerning the country of study, 11 studies were from Asia,11–21 three were from Europe,22–24 two from America25 26 and one from Africa.27
Overview of literature included in the meta-analysis
Meta-analysis results
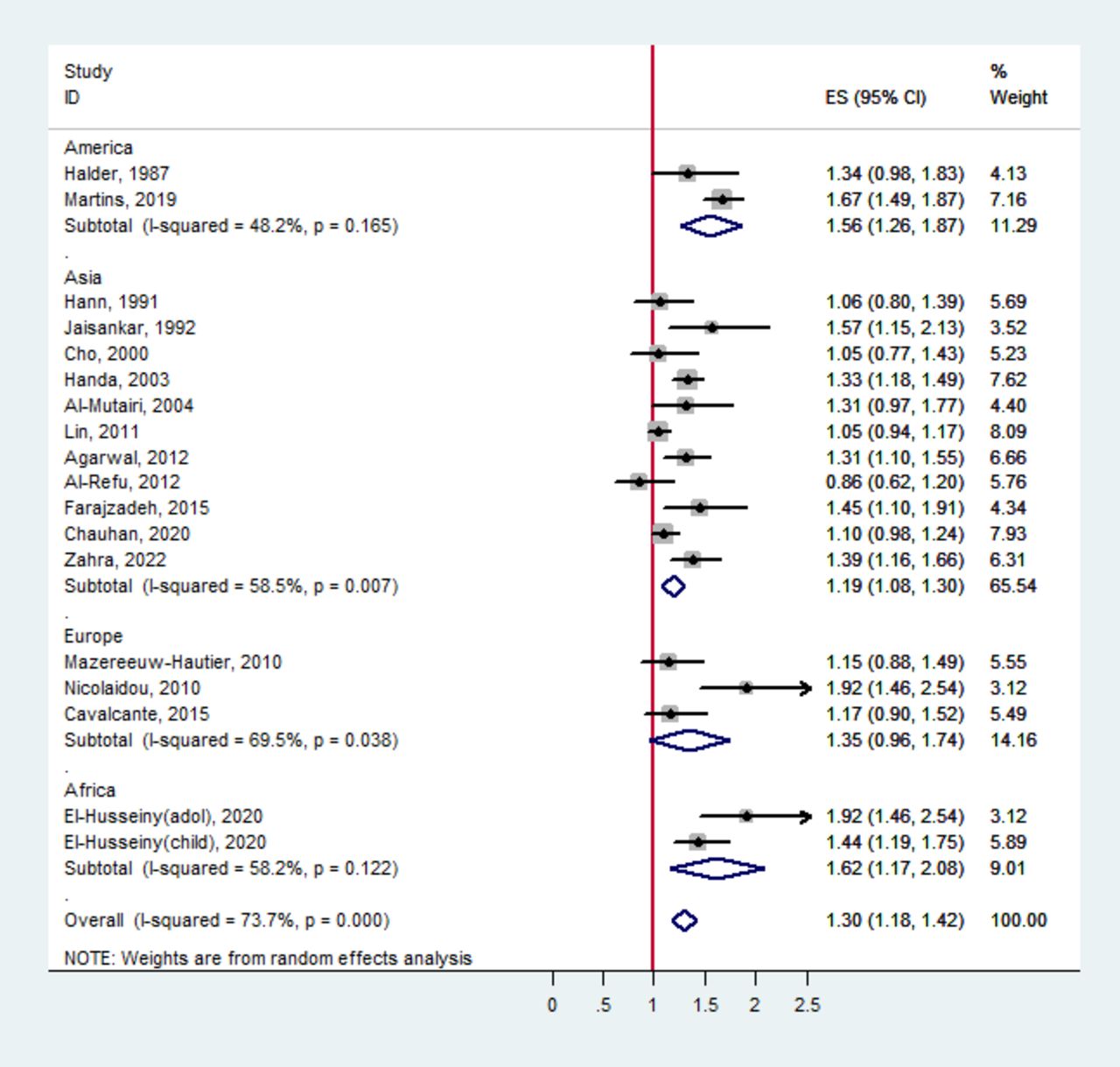
The clinical characteristics of childhood vitiligo are presented in table 2. The meta-analysis of 17 studies with 4365 subjects yielded 2475 women (estimated=56.8%, 95% CI 54.45 to 59.22). In the present study, a female-to-male ratio of 1.3:1 was identified (estimated=1.3%, 95% CI 1.18 to 1.42) (figure 3). Heterogeneity (I2) was large in the female-to-male ratio (I2=73.7%: p<0.001). Therefore, we used meta-regression analysis to investigate potential heterogeneity sources. Meta-regression demonstrated a significant relationship between continents and gender (p=0.038). Africa was reported to have the highest ratio (estimated=1.62%, 95% CI 1.17 to 2.08) in one study (figure 2).

The forest plot of female to male ratio of patients with childhood vitiligo. ES, estimated.
Clinical characteristics of childhood vitiligo worldwide
Age analysis was performed in nine studies involving 2971 vitiligo patients. The results revealed that the average age of patients was 7.47 years (estimated=7.47, 95% CI 5.41 to 9.52) (figure 3).

The forest plot of mean age of patients with childhood vitiligo. ES, estimated.
The most common types of non-segmental vitiligo were vulgaris (estimated = 42.49%, 95% CI 31.11 to 53.87), focal (estimated = 27.21%, 95% CI 20.03 to 34.39) and acrofacial (estimated = 17.8%, 95% CI 12.02 to 23.52) (table 2).
The pooled ratio of non-segmental to segmental was 4.6:1. I2 was calculated to be 83.8%. Africa, with one study (estimated=11.56%, 95% CI −0.98 to 24.10), and America, with two studies (estimated=3.02%, 95% CI 1.54 to 4.50), had the highest and lowest ratios, respectively (figure 4). Using meta-regression, the relationship between continents and vitiligo type was found to be insignificant (p=0.47).
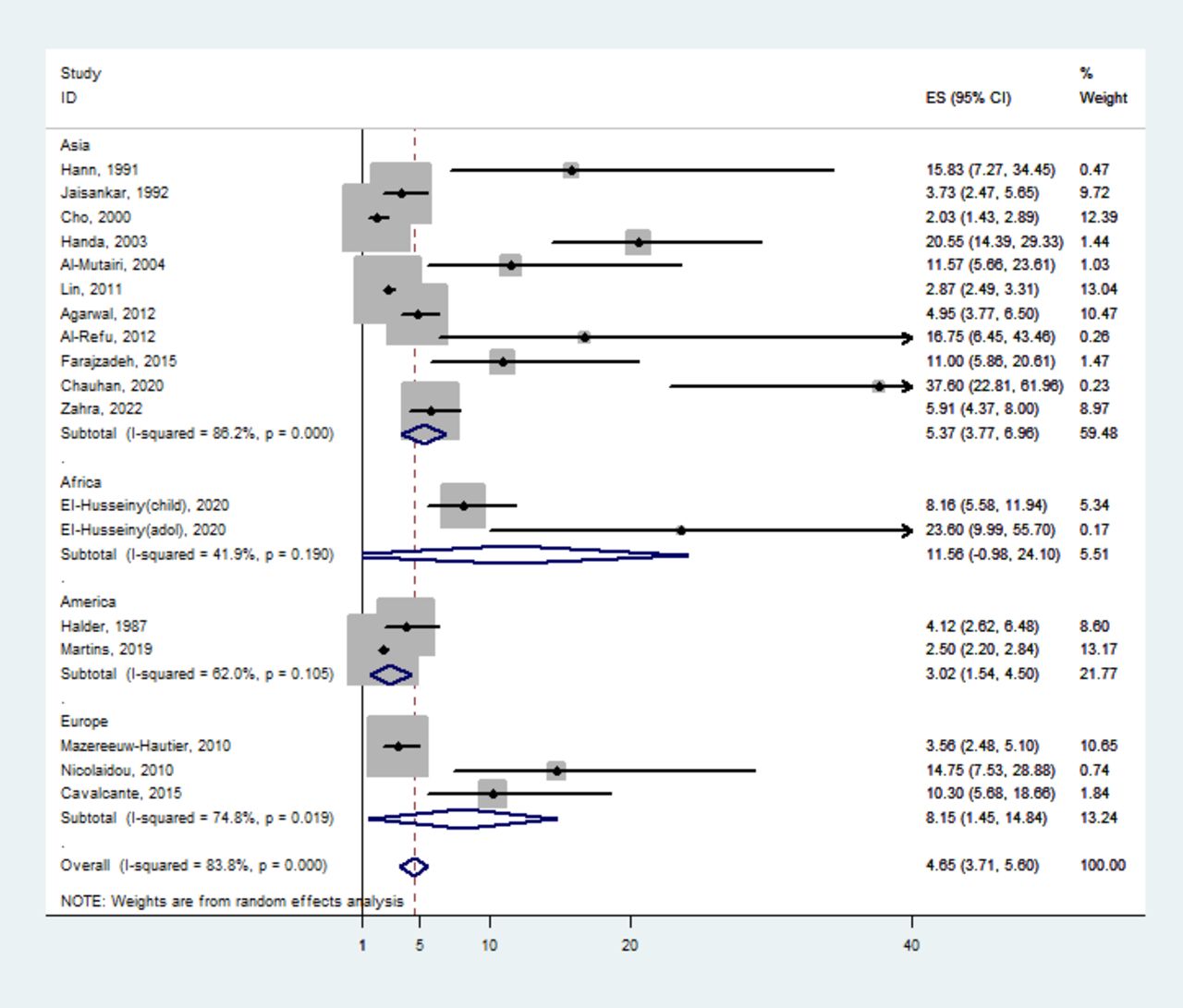
The forest plot of non-segmental to the segmental ratio of patients with childhood vitiligo. ES, estimated.
A positive family history was recorded in 657 patients with childhood vitiligo (estimated=16.88%, 95% CI 13.37 to 20.39). Positive family history varied by continent of study from 13.91% (Asia with 11 studies) to 27.01% (Europe with two studies) (figure 5). Using meta-regression, the relationship between continents and family history was not statistically significant (p=0.11).

The forest plot of positive family history of vitiligo in patients with childhood vitiligo. ES, estimated.
The most common initial lesion sites were the extremities (57.69%), head/neck (46.78%) and trunk (15.62%). Kobner phenomena and leukotrichia were observed in 687 (estimated=25.47%, 95% CI 18.64 to 32.29) and 461 (estimated=18.52%, 95% CI 41.66 to 51.89) patients, respectively (table 2).
Halo nevus (6.59%), atopic and allergic diastasis (6.11%), premature canities (4.97%) and alopecia areata were the most common cutaneous associations in childhood vitiligo (1.08 %). Anaemia (5.84%) and thyroid disorders (5.19 %) were the most prevalent systemic associations (table 2). Stress (estimated=27.41%, 95% CI 7.57 to 47.24) and trauma (estimated=5.62%, 95% CI 4.20 to 7.03) were the most prevalent precipitating factors in patients with childhood vitiligo (table 2).
Publication bias
A visual examination of Begg’s funnel plot revealed no significant asymmetry between studies of childhood vitiligo and patient age. Both Egger’s (p=0.416) and Begg’s (p=0.283) tests indicated that there was no significant publication bias (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Begg’s funnel plot of publication bias analyses.
Discussion
In this study, the most common clinical presentation of vitiligo in children was a school-aged girl with vitiligo vulgaris initiated from the head and neck with a positive family history in about 17% of cases, and the possibility of association with anaemia, thyroid disorders and halo nevus.
According to the findings of this meta-analysis, women predominated over men (female-to-male: 1.3: 1). However, Cho et al 15 reported a near-equal incidence in both sexes, and another study reported the opposite ratio.13 The higher incidence of childhood vitiligo in women can be attributed to the higher prevalence of autoimmune conditions in the female gender, which is indirectly related to the increased stigma of the cosmetic appearance in vitiligo among the parents of the girl child. As vitiligo is generally regarded as a cosmetic condition, medical attention may be sought earlier.21 27
In addition, the meta-regression analysis revealed a significant association between the female predominance of childhood vitiligo and geographical area, with a lower ratio in Asia and Europe than in Africa. In addition to differences in ethnicity, a greater awareness of childhood vitiligo in more developed countries than in Africa may be a contributing factor.
Approximately, 50% of initial lesions occur in the head and neck, according to the results of the systematic analysis. However, the exact interpretation of the data is challenging, but more frequent sun exposure during sports increases the risk of vitiligo in genetically susceptible individuals.21 27 Additionally, this site focuses more on vision and evaluation. Extensive sun exposure generates high levels of oxygen free radicals, which are detrimental to genetically susceptible melanocytes in vitiligo.28 Involvement in the genital region was less common among children. This may be due to less active melanocytes in children under hormonal stimulation, less vulnerability to attack and less friction and loss of melanocytes associated with sexual activity in older children.29
Vitiligo is sometimes preceded by some precipitating factors. According to the findings of the present systematic review, stress and trauma are two common precipitating factors. The higher incidence of trauma as a precipitating factor may bias the correlation between vitiligo and a prior episode of childhood trauma.
The most prevalent cutaneous association in childhood vitiligo was halo nevus, followed by atopic and allergic diastasis and premature canities, respectively.
Genetic factors play an important role in the pathogenesis of vitiligo.13 23 Therefore, positive family histories unrelated to ethnicity and more relevant to an individual’s genetic background can be expected in children.
Heterogeneous studies pose a significant limitation in combining observational studies for the current meta-analysis. We attempted to reduce this heterogeneity by employing relatively narrow inclusion criteria and evaluating the quality of included studies using an NIH protocol. We used meta-regression to explain potential sources of the identified heterogeneity. Another limitation is that only English-language papers were included.
Despite some limitations, the strength of this review stems from its use of established methods for conducting systematic reviews, extensive searching and a combined quality assessment of the included studies.
Finally, the compilation of all available evidence on the clinicoepidemiological pattern of childhood vitiligo will help for better identification of a clinical pattern of disease and modifying potential risk factors.
Conclusion and recommendations
Currently, there is no clear picture of the clinicoepidemiologic pattern of childhood vitiligo worldwide. This article describes the clinical and epidemiologic characteristics of childhood vitiligo. Although gender disparities vary between countries, the findings indicate that vitiligo is more prevalent in female children. Other findings, such as the age of children, the location of lesions, the pattern of vitiligo and family history of vitiligo, were similar in American, Asian, European and African children.
Awareness of the typical pattern of childhood vitiligo in different geographic regions and its associated factors around the world improves clinical disease identification and management. To provide more reliable data in the future, we suggest conducting additional research in diverse geographic regions and community settings.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BAN and SF designed the study and wrote the study protocol. As the first reviewer, BAN and FR performed the study screening, selection, and data collection. MM and FP performed the statistical analysis and drafted the manuscript. MK and SF supervised the research work and was the third reviewer in case of discordance between BAN and FR during study screening and selection. MK, SF, and MM revised the manuscript. All authors revised and approved the final version of this manuscript. BAN is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.