Article Text

Abstract
Background Paediatric clavicle fractures are commonly seen in the emergency department (ED), and the current standard of care is to obtain a radiograph for all suspected clavicle fractures. We are yet to determine whether radiographs add valuable information to clinicians’ assessment and therefore if they are necessary in the management of paediatric clavicle fractures.
Objective To determine whether clinicians can manage paediatric clavicle fractures without radiographs, first by determining the accuracy of clinicians in identifying the presence of a clavicle fracture, and second by evaluating the level of agreement (kappa (κ)) between the ultimate management of children with suspected clavicle fractures and clinicians’ blinded prediction prior to the radiograph.
Methods This prospective study enrolled patients presenting to a paediatric ED with a suspected clavicle fracture. Prior to requesting a radiograph, clinicians completed a standardised form, where they predicted the presence of a fracture and their ultimate management based on their clinical findings, and rated their confidence.
Results Of the 50 patients aged 7.2±3.9 years included, 40 (80%) had a radiologically proven clavicle fracture, and clinicians were able to accurately identify them (sensitivity 93%, positive predictive value 88%). There were five (50%) patients without a radiological fracture that were treated with broad arm sling. Clinicians’ prediction of ultimate management had the highest agreement with the ultimate management of the patient on leaving the ED, compared with clinicians’ prediction of the presence of fracture and the final radiograph findings: κ of 0.88 (95% CI 0.64 to 1), 0.67 (95% CI 0.36 to 0.98) and 0.62 (95% CI 0.30 to 0.94), respectively. Thirty-six (72%) of the clinicians felt comfortable treating without radiographs, and this was dependent on their level of training.
Conclusions Clinicians can identify the presence of a fracture and tend to be overconservative in their management. Despite negative radiological findings, some patients were treated as though they had a fracture, based on clinical judgement. This adds evidence that radiographs are not routinely required for uncomplicated paediatric clavicle fractures.
- clavicle
- fracture
- pediatrics
- emergency department
- x-ray
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Clavicle fractures are commonly seen in paediatric emergency departments.
Obtaining radiographs for suspected clavicle fractures is the standard of care across the majority of departments, but we are yet to determine if they are necessary.
What this study hopes to add?
Clinicians can identify the presence of a fracture from clinical examination alone and tend to be overconservative in their management.
Radiographs do not appear to influence ultimate management or add valuable information to clinicians’ assessment.
Uncomplicated clavicle fractures can be managed without radiographs in a paediatric emergency setting.
Introduction
Clavicle fractures are frequently seen in the emergency department (ED), accounting for approximately 15% of all paediatric fractures.1 2 The standard of care is to obtain a radiograph for suspected clavicle fractures prior to treatment. First-line treatment in most children is conservative management with broad arm sling (BAS).2–4 Past studies have shown that ED clinicians are able to accurately diagnose clavicle fractures from clinical examination alone.1–4 Requesting radiographs may be a habit of emergency practice, as it has not been determined if radiographs add valuable information to clinicians’ assessment and influence their management.1 4–6
A reduction in the number of radiographs would lower overall costs and radiation exposure, as clavicle injuries occur commonly in children.5–8 While the absolute risk to the individual may be low, the cumulative risk from radiographs across this radiosensitive population remains a legitimate concern.9–11 Clinicians must justify any exposure to radiation,9 and it may be considered inappropriate to routinely request radiographs for suspected fractures when they could be managed effectively without, as some studies have suggested.1 4 This is aligned with the current Choosing Wisely campaign, which aims to reduce unnecessary investigations,12 and the Image Gently Alliance, which seeks to improve safe and effective imaging care of children.13
To our knowledge, there has been no prospective study conducted in a paediatric setting only, and none that assessed clinicians’ ability to manage clavicle fractures without radiographs. Furthermore, it is current standard of care across the majority of EDs in the UK and the rest of the world to order clavicle X-ray in all cases of suspected clavicle fractures. Therefore, the aim of this study is to determine if clavicle fractures can be managed in the paediatric ED setting without radiographs.
Materials and methods
Setting and participants
The study was conducted in the ED at the Royal Hospital for Sick Children, a tertiary teaching hospital in Edinburgh, UK, serving urban and suburban populations. The ED has an annual census of approximately 40 000 visits. The clinicians participating in this study included ‘Junior trainees’ (doctors with ≤4 years of experience), ‘Senior trainees’ (doctors with ≥5 years of experience), ‘Specialty doctors’, ED consultants and emergency nurse practitioners (ENPs). Patients seen by ‘Junior Trainees’ or ENPs were reviewed by a senior prior to discharge. Participants received no extra training and current practice was not altered.
Design
This prospective study enrolled a convenience sample of 50 patients between 9 May and 19 September 2012. All children who presented to the ED with suspected clavicle fractures were included in the study, unless the radiograph was performed when suspecting non-accidental injury or in children over the age of 16. Parents verbally consented to take part in the study.
After clinical examination, clinicians were required to fill in a standardised study form before requesting a clavicle radiograph (online supplementary appendix 1). Clinicians were blinded to the radiological findings when completing the form, as radiographers were instructed not to perform an X-ray without a completed survey form. The clinicians circled on the form if they thought there was a fracture, no fracture or if they were unsure. Then, they rated how confident they were on a 10 cm Visual Analogue Scale (VAS), which was limited by the terms ‘certain no fracture’ and ‘certain of fracture’. Clinicians answered if they felt comfortable in managing the patient without a radiograph, and if not why (suspected complication; unsure localisation; lack of experience; for prognostic value; or other). They were asked how they would treat the patient if there was no radiograph available (analgesia and BAS; analgesia and advice to mobilise; referral to orthopaedics; or other). The radiograph findings were reported by consultant radiologists, and we obtained patients’ ultimate treatment through TrakCare, the National Health System Lothian patient management system. Missed cases were identified using TrakCare to obtain all clavicle X-rays requested over the study period.
Supplementary file 1
We provisionally assumed that the treatment for clavicle fractures is with a BAS and analgesia, as it is the standard of care for uncomplicated fractures in most EDs across the world. We defined complicated fractures as those that required surgical intervention, for example, open fractures or those with neurovascular injury.
Outcomes
The overall aim of the study was to determine whether clinicians can manage paediatric clavicle fractures without the use of radiographs. Our primary outcome was to determine whether clinicians can accurately identify the presence of a fracture from clinical assessment alone. To measure this, the sensitivity, specificity, and positive predictive value (PPV) and negative predictive value (NPV) were calculated. Our secondary outcome was to compare the level of agreement between the patient’s ultimate management on discharge from the ED and the clinician’s blinded predictions (prediction of the presence of fracture or not, and prediction of ultimate management), prior to requesting a radiograph, as well as the final radiological reports. This agreement was measured using the kappa statistics (κ) for inter-rater reliability. Lastly, our third outcome was to determine whether clinicians felt comfortable in treating patients without radiographs, according to their level of training, and the confidence of their assessment of the presence of a fracture on the VAS.
Data analysis
The data were entered into Microsoft Excel V.2008 and analysed using IBM SPSS Statistics V.21.0. Age is presented as mean and SD. The CI was calculated for 95% of our results using a template based on the Wilson method of proportions using the Confidence Interval Analysis V.2.2 software.14 SPSS was used to calculate the κ coefficient. Guidelines have suggested that values should be higher than 0.7 to claim excellent agreement; however, we have chosen a value greater than 0.75 to account for the subjective nature of clinicians’ predictions.14 15
Results
Over the 134-day study period, 83 cases of trauma to the clavicle were seen in which a radiograph was obtained (figure 1). From these, 51 patients were enrolled. There was one patient with a completed study form that was excluded from the study as he was managed via telephone consultation. The mean age of the study population was 7.2±3.9 years; 22 patients were under the age of 5 (44%) and 10 (20%) were above 10 years of age. The majority of the patients were male (34, 68%). Among the 50 patients, 40 (80%) had a clavicle fracture reported on radiograph (table 1). Forty-five (90%) patients were treated with a BAS and analgesia, including all 40 patients with a fracture, but also 5 patients without a fracture. Five (10%) patients were discharged with analgesia and advice to mobilise, all without fracture (table 2). There were no radiographs performed in the context of non-accidental injury, no open fractures, patients with neurovascular injury and/or patients who required surgical interventions.
Comparison of clinicians’ predictions and radiological reports (n=50)
Comparison of predicted and ultimate management of patients (n=50)

Flow of patients in the study.
Identification of fractures
After clinical examination alone, clinicians thought there was a fracture in 42 (84%) of the 50 enrolled patients, with 37 of those cases radiologically proven clavicle fractures. Clinicians predicted there were no fractures on one occasion only, and there were no radiological fractures reported for that patient. They were unsure in seven patients, and three out of those (43%) had radiologically reported fractures (table 1). The sensitivity and specificity of clinicians to predict the presence of fracture were 93% (95% CI 80 to 97) and 50% (95% CI 24 to 76), respectively. The PPV and NPV of the clinicians were 88% (95% CI 75 to 95) and 62% (95% CI 31 to 86), respectively.
Patients’ ultimate management
Clinicians predicted a treatment of BAS and analgesia in 46 patients, and ultimately 45 of these patients were treated with BAS and analgesia (table 2). All four patients for whom clinicians predicted a treatment of analgesia and advice to mobilise were treated this way. Thus, the sensitivity and specificity of clinicians to predict the ultimate management after their clinical evaluation, but before they had seen the radiograph, were 100% (95% CI 92 to 100) and 80% (95% CI 38 to 96), respectively. The PPV and NPV values of the clinicians were 98% (95% CI 89 to 100) and 100% (95% CI 51 to 100), respectively.
Clinicians’ prediction of the presence of a fracture was also a good predictor of ultimate management. There were 41 patients who were predicted to have a fracture by the clinicians and were treated with a BAS; therefore, only one was treated with analgesia and advice. Clinicians predicted there would be no fracture or were unsure on eight occasions, and treated five (63%) of these with advice on mobilisation and analgesia. The accuracy of clinicians’ prediction of the presence of a fracture in predicting ultimate management was the following: sensitivity and specificity, 93% (95% CI 82 to 98) and 83% (95% CI 44 to 97), respectively; and PPV and NPV, 98% (95% CI 88 to 100) and 62% (95% CI 31 to 86), respectively.
The radiograph findings predicted ultimate management with good accuracy. All of the 40 patients with a radiological fracture were treated with BAS and analgesia. However, there were five patients without a fracture (50%) who were treated with BAS and analgesia. The accuracy of the radiograph findings in predicting ultimate management was the following: sensitivity and specificity, 89% (95% CI 76 to 95) and 100% (95% CI 57 to 100), respectively; PPV and NPV, 100% (95% CI 91 to 100) and 50% (95% CI 24 to 76), respectively.
Level of agreement with patients’ ultimate management
All three predictors of ultimate management had a good level of agreement, with κ values of between 0.62 and 0.88. Clinicians’ predictions of ultimate management had excellent agreement with ultimate management (table 3).
Level of agreement in predicting ultimate management
Level of comfort of clinicians
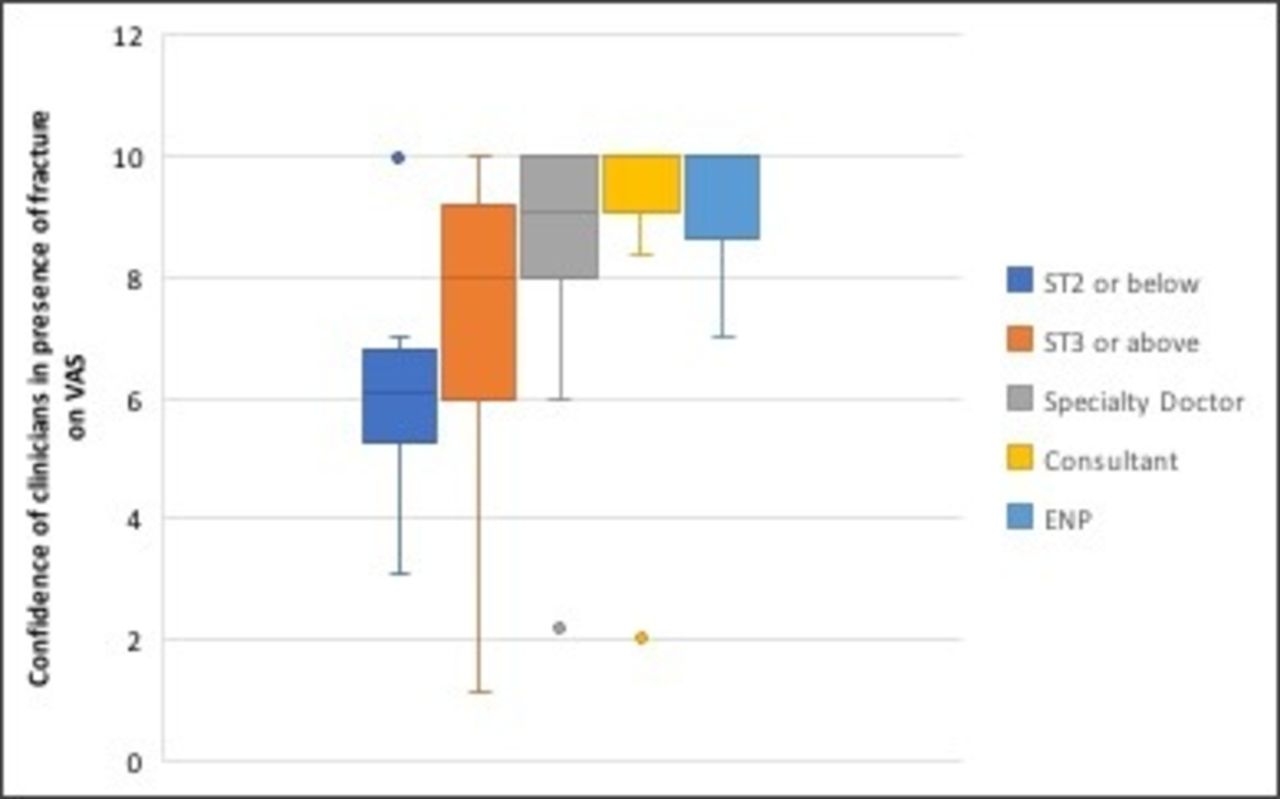
Clinicians stated they would have felt comfortable treating patients without radiographs on 36 (72%) occasions. All six junior trainees who participated in the study felt uncomfortable treating the patient without a radiograph because they all felt they lacked experience. Figure 2 illustrates that the more experience clinicians had, the more confident they felt treating patients without a radiograph when the median VAS was expressed for each category of clinicians’ experience.
{kind=link}
{kind=link}
Median confidence of all clinicians, scored on a VAS (0–10), in predicting a fracture prior to radiograph. ENP, emergency nurse practitioner; VAS, Visual Analogue Scale.
Missed cases
A further 32 patients who had a radiograph for suspected clavicle fracture during the study period were identified. Comparative data were obtained between the enrolled and non-enrolled groups. There was similar age and sex distribution. Furthermore, there were no complications or surgical interventions in either group. Among the 32 patients not enrolled, radiologists reported a fracture on 24 (75%) occasions, and 29 (91%) were treated with a BAS including all patients with a fracture. There were five patients (16%) in the non-enrolled cohort who were treated with a BAS despite no radiological evidence of fracture.
Discussion
Although the current standard of practice is to obtain a radiograph for every suspected clavicle fracture, our study supports that X-rays do not add any valuable information to clinicians’ assessment in the emergency paediatric setting. Indeed, clinicians can accurately identify clavicle fractures from clinical assessment alone and tend to be overconservative in their management, which is comparable with other studies.1–4 Furthermore, we demonstrated an excellent level of agreement between clinicians’ predictions of the ultimate management, prior to seeing the radiograph, and the ultimate management of the patient. Radiographic findings had good agreement with ultimate management; however, clinicians’ predictions had higher kappa values. It seems that radiographic findings did not influence clinicians’ ultimate management when there was no radiological fracture, as there were patients treated with BAS despite negative X-rays findings. They based this management on the diagnosis of ‘clinical fracture’, which is comparable with other studies which suggest paediatric fractures may not always be apparent on initial X-rays.1 4 Interestingly, clinicians’ certainty in their judgement was high regardless of whether they felt comfortable treating the patient without radiograph or not. It appears that the more experienced the clinician, the more comfortable they felt.
Two prospective studies have concluded that physicians can accurately predict the presence of a clavicle fracture without a radiograph; however, none to our knowledge have been conducted in a paediatric emergency setting only.1 4 In one of the studies, clinicians identified all 94 of the radiologically proven fractures,1 and in the other they identified 50 out of 51 fractures (98%).4 Studies have suggested the use of point of care ultrasound (POCUS) in the management of children with clavicle fractures.3 16 These studies required provision of formal training to clinicians who were not blinded, therefore introducing operator and confounding bias. Some studies have highlighted the high sensitivity of POCUS in detecting complications such as haemothorax and pneumothorax.17 18 Combining clinical examination and POCUS of the clavicle and chest may be an alternative to X-ray, especially in complicated cases of clavicle fractures.
It is probable that patients and their families prefer or expect radiographs in the management of a suspected clavicle fracture. However, studies suggest the opposite, including those in both paediatric and adult populations.5 19–21 The multicentre trial evaluating the use of the ‘Low Risk Ankle Rule’ demonstrated that this validated clinical decision rule has reduced ankle radiography significantly and safely without change in patient or clinician satisfaction.5 Similarly, the ‘Ottawa Ankle Rule’ did not cause a decrease in patient satisfaction, despite a reduction in X-rays.20 21
Our data indicate that clinicians are guided by their clinical examination rather than the radiographic findings. While omitting radiographs could potentially lead to ‘over-treatment’, placing a child’s arm in BAS for short periods poses little harm to the child and provides relief from pain in patients who have not sustained a fracture in any case. Indeed, at our institution, we have reduced the use of radiographs for traumatic clavicle injury by 86% in the 4 years after this study was conducted, with no evidence of mismanagement or complication (995 radiographs performed between February 2008 and August 2012 compared with 136 performed between November 2012 and November 2016).
It is likely that radiographs are required for very young patients, in open fractures, in cases of non-accidental injury, in those with neurovascular compromise or those that cannot be adequately clinically assessed.22 We suggest further clinical studies to ultimately develop clinical decision tool to help emergency clinicians in deciding when to order X-rays.
Limitations
This study had some potential limitations. It is limited by a small group of patients and conducted in a single tertiary paediatric hospital, thus may not be representative of other emergency settings. Furthermore, all patients had non-complicated clavicle fractures. We therefore could not comment on how to identify rarer cases that would require surgical intervention. We believe that routine radiographs are common practice and conservative management is the first-line treatment in most EDs.1 2 4 16 23 The study aimed to obtain consecutive sampling, but some patients were not enrolled due to recruitment failure. Despite this, we have no reason to believe that the patients not enrolled were different from those included. Another limitation was that the study could not determine whether the clinician’s level of experience would be problematic in managing patients if radiographs were omitted. A relatively small number of clinicians participated in the study and perhaps a deeper analysis of their level of training would be appropriate. This could be potentially important for non-paediatric EDs. However, less experienced clinicians still appeared to have accurate predictions, despite being less confident. Nevertheless, even if less experienced clinicians were to overtreat more patients without fractures, we would still contend the large number of radiographs omitted would justify the brief and minor inconvenience of a BAS in a small number of patients.
Another limitation is that clinicians were making theoretical predictions and may have responded differently if radiographs were actually omitted. We acknowledge that the decisions on management prior to and after the radiograph are not independent. However, it is our opinion that it does not invalidate the conclusion that suspected clavicle fractures can be safely managed without radiographs.
Conclusion
The current literature and our study demonstrate that radiographs can be omitted in the routine assessment of suspected clavicle fracture in children. To our knowledge, our study is the first to demonstrate that uncomplicated clavicle fractures can be managed without radiographs in a paediatric emergency setting. We contend that in the context of suspected traumatic clavicle injury in a cooperative child, in whom surgical intervention is not anticipated, clavicle radiographs are not required.
Acknowledgments
The authors would like to acknowledge the work of Dr Margaret MacDougall for the earlier version of this manuscript.
References
Footnotes
Contributors M-PL and PL led the project and were involved in all parts of the study, including planning, acquisition of data, analysis and interpretation of the work, and drafting the manuscript as well as the final version of this manuscript. MJ had substantial contributions to the acquisition of data, and revising various versions as well as the final version of this manuscript. SG provided significant contributions to the interpretation of the data for the work, and revising the various versions as well as the final approval of this manuscript. BB was heavily involved in the statistical analysis of the data, contributed a significant amount to the interpretation of the data, writing of all parts of the manuscript, and editing multiple versions including the final approval of this manuscript. All authors agree to be accountable for all aspects of the work and believe it is an honest and valid work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Royal Hospital for Sick Children, Edinburgh, Scotland, UK. The ethics committee of the University of Edinburgh approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.