Article Text

Abstract
Background Mask leak and airway obstruction are common with mask ventilation in newborn infants, leading to suboptimal ventilation. We aimed to perform a pilot study measuring respiratory mechanics during one-person and two-person mask ventilation in preterm infants at birth.
Methods Infants less than 30 weeks’ gestation were eligible for the study. In the two-person method, one person holds the mask in place and the other provides positive pressure ventilation compared with the standard one-person mask hold. A respiratory function monitor was used in line with a T-piece resuscitator to measure mask leak and airway obstruction. Deferred consent was obtained.
Results Twenty-five infants were recruited. The mean (SD) birth weight was 920.4 g (188.3), and mean (SD) gestational age was 27.3 weeks (3.0). Percentage mask leak was higher in the one-person mask method (26.4±18.5) compared with the two-person mask method (17.6±9.3) (p=0.018). The mean (SD) expired tidal volume (VTe, mL) in breaths with leak was 3.9 (1.57) in the one-person method compared with 3.05 (1.0) the two-person method (p=0.31). A significantly lower mean (SD) end-tidal carbon dioxide (EtCO2, mm Hg) was measured at 25.3 (9.9) in breaths with mask leak, compared with 30.8 (12.1) in breaths without leak. The breaths with airway obstruction had lower mean EtCO2 (25.9 vs 30.8, p=0.003) and lower mean VTe (1.71 vs 6.95, p<0.001).
Conclusion Mask leak and airway obstruction are common in resuscitation of preterm infants at birth. The use of the two-person mask technique is effective and it could be a useful option if mask ventilation with the one-person method is not effective.
Trial registration number ACTRN12614000245695.
- Neonatology
- Resuscitation
Data availability statement
All data relevant to the study are included in the article or uploaded as an online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Mask leak and airway obstruction are common in preterm infants and they often not recognised by the resuscitator.
A respiratory function monitor has been identified to be feasible at resuscitation for preterm infants at birth.
A two-person method of mask ventilation leads to better tidal volume and less mask leak in a manikin model.
WHAT THIS STUDY ADDS
A two-person method of mask ventilation is feasible in resuscitation of preterm infants at birth.
Significant airway obstruction and mask leak leading to reduction in tidal volumes are common with mask ventilation.
A two-person method of mask ventilation could be an effective option for clinicians if mask ventilation is not effective with a one-person method.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our results show that the use of two-person mask ventilation in resuscitation of preterm infants at birth is feasible.
The two-person method of mask ventilation needs to be evaluated in a larger group or cohort.
Introduction
Extreme preterm infants need ventilatory support to establish lung aeration at birth. However, escalation of ventilatory support could inadvertently induce barotrauma and/or volutrauma.1 Recognition of lung aeration prior to intubation is vital but reliable assessment of this at birth is difficult, even by an experienced hand.2
Some infants require positive pressure ventilation (PPV) to establish sufficient alveolar ventilation and functional residual capacity to correct hypoxia. Significant mask leak and airway obstruction are very common, reducing effective alveolar ventilation and thus effectiveness of PPV.3 4 Recognition of mask leak at resuscitation is clinically difficult.5 Studies have highlighted the finding of upper airway obstruction (hyperflexion/hyperextension of the neck) as a frequent event in extremely premature infants, which can coexist with a mask leak and potentially render the PPV ineffective.6
Given the difficulty with recognising mask leak or airway obstruction during PPV without a complex respiratory mechanics’ monitor, a suboptimal response is likely to be attributed to ‘bad lungs’ rather than poor mask technique, resulting in peak inflation pressures being increased. Observation of chest rise is inadequate for estimating appropriate tidal volumes.7 Assuming the endotracheal tube is well placed, this situation may expose the premature infant to excessive tidal volumes and minute ventilation. These are both directly injurious to fragile immature lung tissue and cause indirect injury to the brain via the effect of hypocarbia, inducing a reduction in cerebral blood flow.8
Finer et al demonstrated that more than 70% of extremely premature infants needing mask ventilation had a median of 14 breaths with airway obstruction before adequate alveolar ventilation was established.9 Woods et al demonstrated leak at the face mask resulted in inadequate ventilation, with operators unable to reliably detect leak during PPV.10 A study by Tracy et al, using a two-person technique for mask ventilation in a manikin model, demonstrated that mask leak was halved compared with the standard one-hand technique.11 This was the first study to support the use of two-person mask ventilation in newborn infants. The UK Resuscitation Guidelines (2015) support the use of a two-person mask technique for neonatal resuscitation if ventilation is not effective.12 The two-person technique was reported in the adult literature as early as 1985, by Jesudian et al and Thomas et al who studied the technique on an adult manikin and reported higher tidal volumes with this method.13 14 The ‘EC-Clamp’ technique with a two-handed jaw-thrust technique has been described to deliver significantly higher minute ventilation in adults as compared with a one-hand technique.15
The aim of this study was to compare one-person versus two-person methods of mask ventilation in preterm infants and to measure respiratory mechanics, including mask leak and airway obstruction, using these different methods of mask hold.
Methods
The study was conducted from June 2015 to February 2016. The pilot study was prospectively registered with Australia New Zealand Trial Registry (ACTRN12614000245695) on 7 March 2014. Eligible infants were randomised to either a one-person mask-hold method (the current standard technique)—in which the resuscitator holds the mask in place with one hand using a two-point top hold and the other hand provides PPV—or the two-person method in which one person holds the mask on the upper rim at four points, applying downward force with a jaw-thrust chin lift, and the other person provides the PPV. If needed clinically, PPV was supplied using a T-piece resuscitator (Neopuff, Fisher & Paykel Healthcare, Auckland, New Zealand), with start settings of: 25 cm H2O for peak inflation pressure, 5 cm H2O for positive end expiratory pressure; and fresh blended gas flow of 10 L/min at 30% FiO2 to Neopuff. A respiratory function monitor (RFM) (Respironics NM3, Philips Healthcare, Best, The Netherlands) was used in line with the mask to measure respiratory mechanics. This includes an end-tidal carbon dioxide (EtCO2) monitor with an accuracy of 2 mm Hg at 0–40 mm Hg. Airway obstruction was defined as a 75% reduction in expired tidal volume compared with the baseline of 10 inflations prior to the obstructed inflation (figure 1A). Percentage mask leak was defined as: (tidal volume inspired (VTi)−tidal volume expired (VTe)/VTi×100); and a mask leak of >75% was considered significant (figure 1B).16 The operators were blinded to the RFM.

(A) Airway obstruction during mask ventilation in infant at 28 weeks’ gestation. The solid arrow on the top graph depicts reduction in gas flow with simultaneous reduction in EtCO2 (broken arrows) and tidal volumes. (B) Mask leak in another infant at 28 weeks’ gestation with the solid line showing inspiratory flow towards the infant but very little coming out. The broken arrow shows the reduction in measured inspiratory pressure with simultaneous reduction in EtCO2 and tidal volumes.
Participants
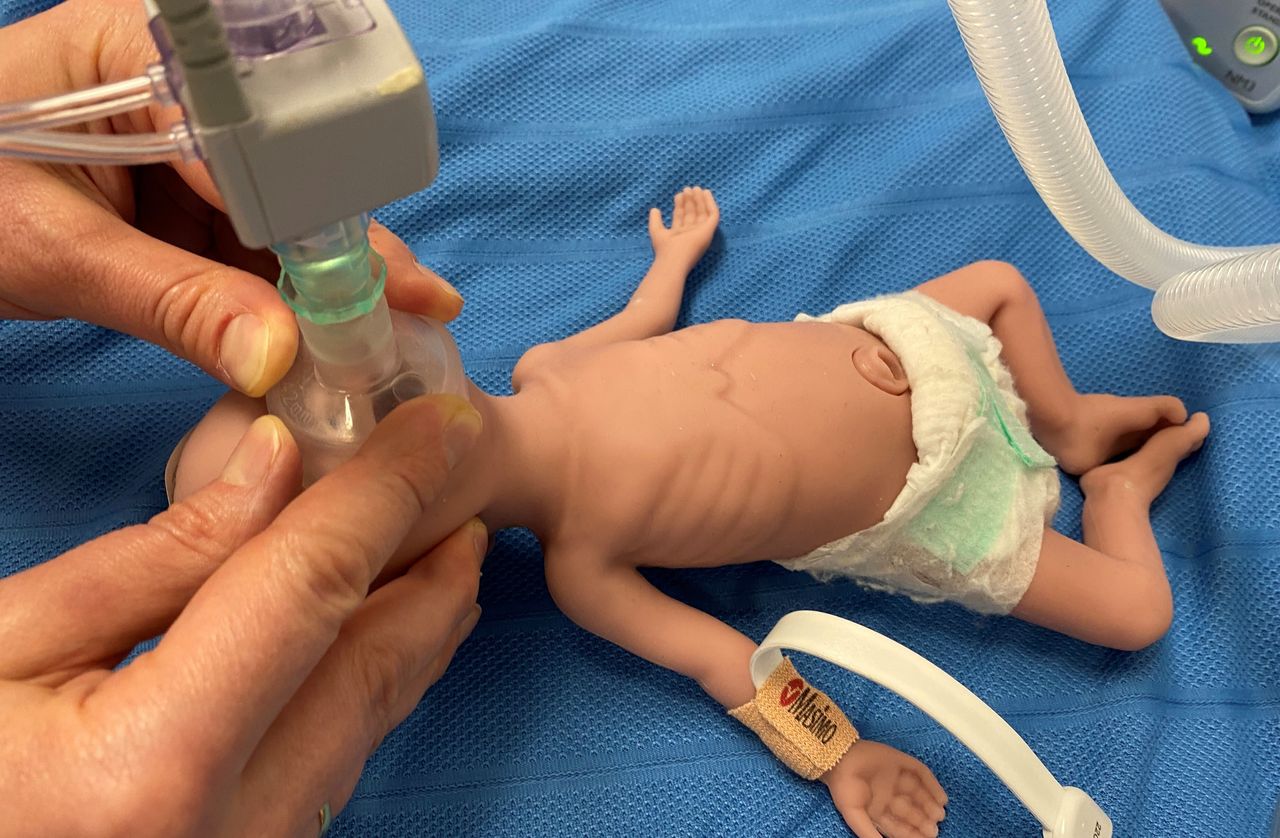
All infants born prematurely at less than 30 weeks’ gestation were eligible for the study if they needed respiratory support in form of mask ventilation. The decision to provide mask ventilation included apnoea requiring PPV, persistent desaturation and increased work of breathing. A round mask (35 or 42 mm external diameter) was used and the resuscitators were senior neonatal fellows who were trained to perform different techniques of mask ventilation (figure 2).
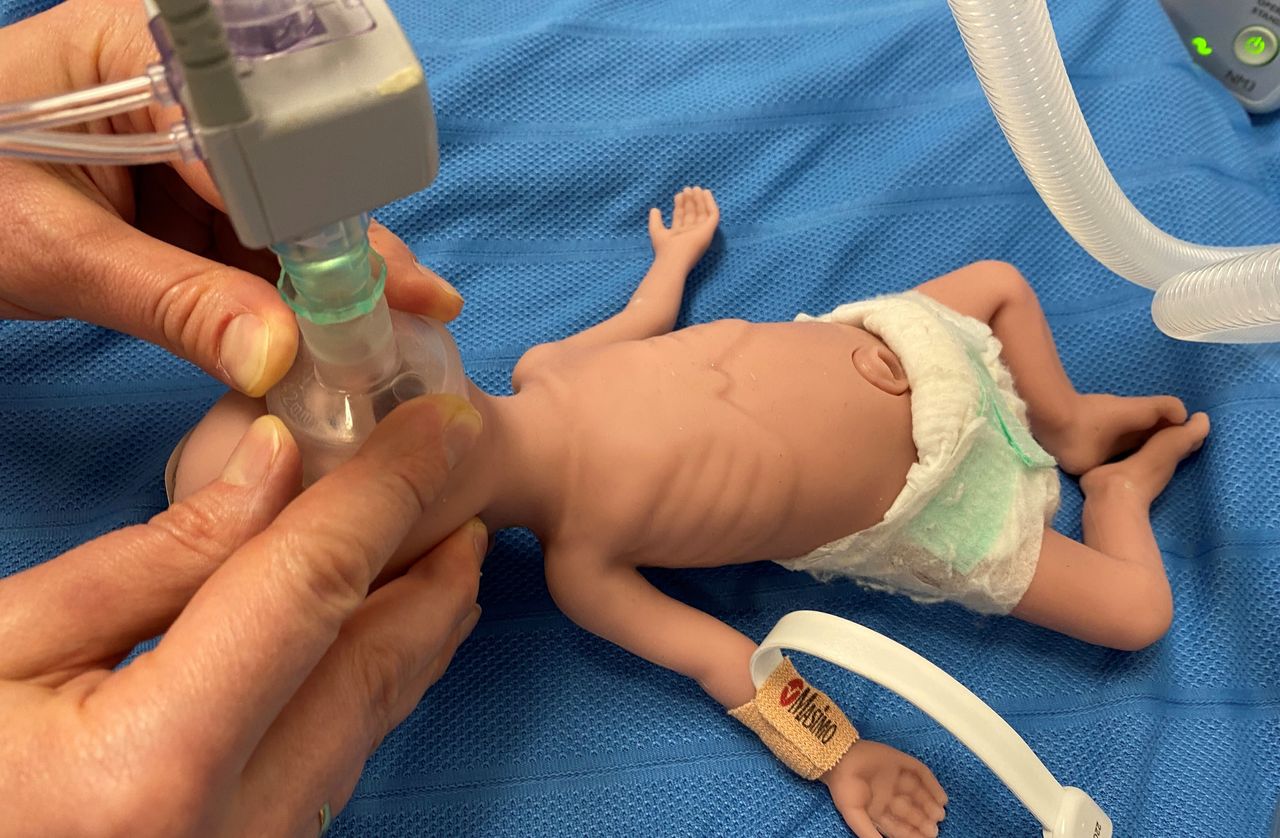
A two-person technique of mask ventilation.
Exclusion criteria
The exclusion criteria included neonates with lethal congenital anomalies, upper airway anomalies and unavailability of the research team.
Outcome measures
The primary outcomes included mask leak and airway obstruction. The secondary outcome was need for airway intubation in the delivery suite with EtCO2.
Randomisation
The infants were block randomised (1:1) using a sealed opaque envelope with computer-generated random numbers. This was a pilot study and not powered directly to detect significant changes in the primary outcomes. Parental consent was sought, if possible (from women in the antenatal ward), but retrospective consent was sought for infants born in emergency situations.
Parent and public involvement
There was no involvement of parents or the public, in the concept, design, reporting or dissemination plans of the research.
Statistical analysis
Statistical Analysis was performed using Stata V.MP18 (Stata Corp. College Station, Texas, USA). The medians and SD of the number of breaths with mask leak and airway obstruction during ventilation were computed for the one-person and two-person method groups. A number of breaths were compared rather than proportion of leak due to small sample size. Between groups, differences in the unadjusted mean number of breaths with mask leak and airway obstruction were investigated using two-sample t-tests. These differences were further investigated via the use of negative binomial regression models including offset terms, to account for each participant having been observed for a different number of breaths. These models were used to compute the adjusted mean differences between the groups. Mean differences between the one-person and two-person method groups for physiological parameters, adjusting for mask leak and airway obstruction, were calculated using linear-mixed models. Paired t-tests were used to compare physiological parameters in breaths with and without mask leak and airway obstruction. A significance level of p<0.05 was used for all analyses.
Results
Of the 60 eligible infants, 30 infants were recruited and 30 were excluded due to unavailability of the research personnel. The data was unavailable for five infants. Thirteen infants were randomised to the two-person method. The mean birth weight was 920.4 g (±188.3) and mean gestational age was 27.3 weeks (±3.0). Fifteen infants were male infants and 60% received a complete course of antenatal steroids.
Comparison of one-person versus two-person mask ventilation
There were no significant differences in birth weight, gestational age, mode of delivery, antenatal steroids, 1 and 5 min Apgar scores between the groups. Seven infants were intubated at birth in one-person versus eight in two-person method group (p=0.87). A mean (SD) total of 161.3 (96.55) inflations were analysed (146.6 one-person method and 174.8 two-person method). The median (IQR) VTe was 6.4 mL (5.2–7.4) in the one-person method group compared with 4.7 (3.9–7.4) in the two-person group (table 1). The median (IQR) VTe with leak was 3.9 mL (2.9–4.7) in the one-person method group compared with 3.1 (2.3–3.6) in the two-person method (p=0.05), whereas the median VTe in breaths with obstruction was 1.8 (1.6–1.8) and 1.8 (1.5–1.9) between groups (p=0.57).
Comparison of one-person and two-person method of mask ventilation
The adjusted mean (SD) inflations with leak were significantly higher in the one-person method group (26.5±18.6) versus the two-person method (17.7±9.3, p=0.018). The mean (SD) breaths with obstruction were similar between the groups (22.9 vs 27.4, p=0.315). A number of consecutive breaths with mask leak and airway obstruction were also similar between groups (table 2). The SD for number of breaths with airway obstruction was large due to two outliers with 83 out of 182 and 86 out of 319 breaths with airway obstruction.
Difference between one-person and two-person methods of mask ventilation for breath-to-breath occurrence of mask leak and airway obstruction
Analysis of differences between two-person versus one-person methods on VTe and EtCO2, adjusted for mask leak and airway obstruction showed no statistical significance. The mean difference (95% CI) in VTe was −1.55 (−3.84 to 0.75) adjusted for mask leak and −0.86 (−1.96 to 0.33) adjusted for airway obstruction. The analysis of EtCO2 showed a mean difference (95% CI) of 4.83 (−3.65 to 13.32) adjusted for mask leak and 4.26 (−4.04 to 12.57) adjusted for airway obstruction.
Comparison of breaths with leak and without leak demonstrated significant difference in mean VTe, mean oxygen saturation, EtCO2 and heart rate (table 3). The mean VTe was 6.76 (3.42) in breaths without leak compared with 3.47 (1.39) in breaths with leak. Similarly, the mean VTe was 6.95 (2.97) in breaths without obstruction compared with 1.72 (0.19) in breaths with obstruction. The mean EtCO2 was higher in breaths without mask leak (30.89 vs 25.39, p=0.002), and in breaths without obstruction (30.81 vs 25.98, p=0.003).
Comparison of physiological parameters in breaths with mask leak and airway obstruction
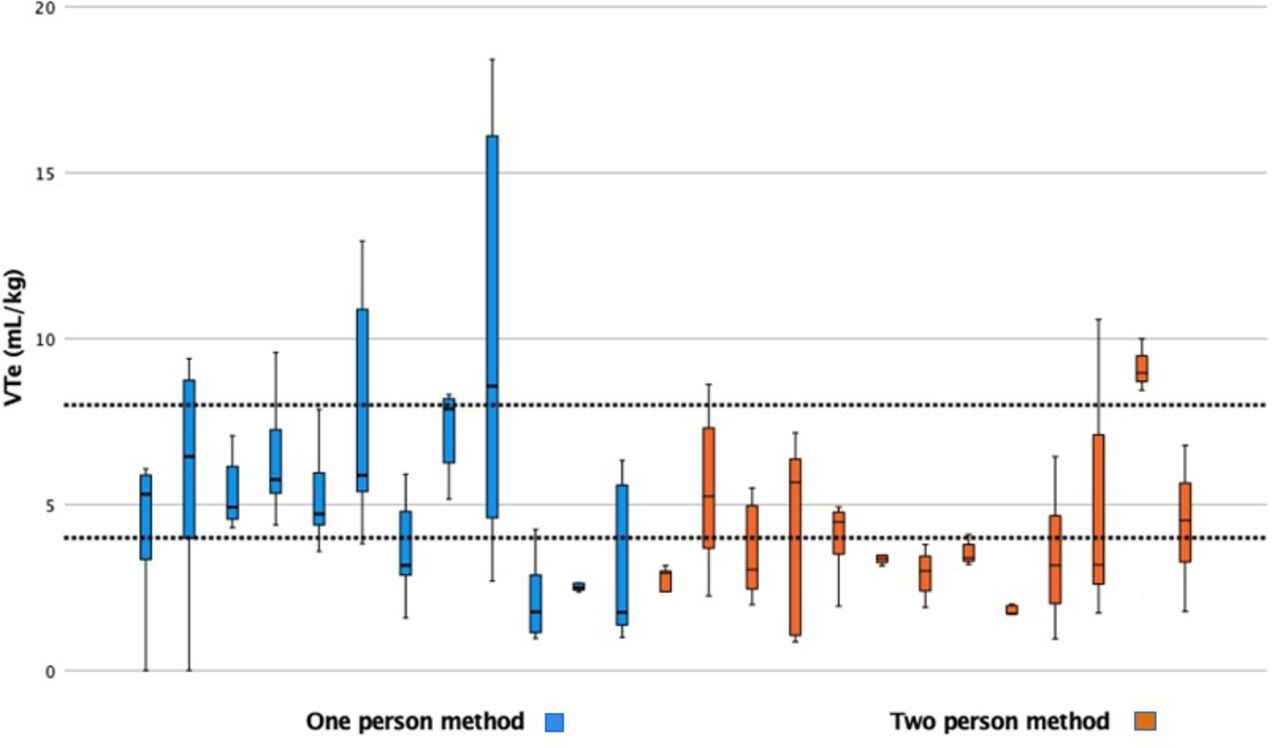
Table 4 compares the respiratory parameters in infants who were intubated and non-intubated at birth. There was no difference in mask leak and airway obstruction. There were significant numbers of infants with mean VTe outside the preferred target of tidal volume (4–8 mL/kg) as shown in figure 3.
Mask leak and airway obstruction in infants intubated versus non-intubated at birth

{kind=link}
{kind=link}
{kind=link}
Graph displaying individual patient mean tidal volume expired (VTe) mL/kg using one-person and two-person methods, with the area between the horizontal dotted lines depicting the preferred VTe (4–8 mL/kg) for individual infants.
Discussion
We demonstrated that there is significant airway obstruction and mask leak in extreme preterm infants resuscitated at birth in the delivery suite. Our study was a pilot study and hence not powered to show significant differences in respiratory parameters and short-term ventilator outcomes, although it does demonstrate significant differences in VTe in breaths with airway obstruction and mask leak. While mask leak and airway obstruction are reported in the literature, our study prospectively demonstrated and quantified the frequency and severity of these events in extreme preterm infants at birth. As transition at birth is a complex process in these preterm infants, provision of optimal airway support is extremely important.
Mask leak is not routinely recognised without specialised volume measurements in resuscitation and potentially reduces alveolar ventilation and thus the effectiveness of the mask PPV at resuscitation. Foglia et al reviewed the respiratory function data in infants at 23–27 weeks’ gestation as post-hoc analysis of the sustained inflation trial.6 They reported significant mask leak (15% of breaths) and airway obstruction (17%) in infants receiving sustained inflation and 3% leak with 17% obstructed breaths in infants receiving PPV.
Our data reflects significant airway obstruction and mask leak in infants receiving mask ventilation. The tidal volumes vary a lot and are quite often outside the target range. In a study of infants under 29 weeks’ gestation, Murthy et al reported lower expired tidal volumes (mL/kg) in infants receiving mask ventilation (1.6, range 0.2–13.3) compared with infants resuscitated via endotracheal tube (2.8, range 0.2–9.9).17 The lower EtCO2 (kPa) was recorded (0.36, range 0–1.8) with mask ventilation compared with endotracheal tube (0.2, range 0–0.9), suggestive of mask leak and/or airway obstruction. This was comparative to our study, with lower EtCO2 in infants with significant mask leak and airway obstruction.
Yang et al prospectively reviewed RFM data in infants under 32 weeks’ gestation receiving PPV.18 They reported mask leak in 32% and airway obstruction in 12% of inflations. They used the mask adjustment, reposition airway, suction mouth and nose, open mouth, pressure increase and alternative airway as intervention, although it was not enough to provide adequate ventilation, with worsening of airway obstruction in four out of five instances. They also reported inflations with low tidal volumes, and only small numbers were associated with bradycardia. Although our study had a small sample size, we demonstrated a significant number of breaths with leak associated with lower heart rate.
Various methods to overcome mask leak and airway obstruction are reported in the literature. A report by Kamlin et al of infants <34 weeks’ gestation confirmed the frequency of airway obstruction with PPV and use of oropharyngeal airways.19 A higher incidence of airway obstruction was noted with use of the oropharyngeal airway. Davidovic et al compared the mean tidal volumes per weight and peak pressures generated by the one-person and two-person techniques of bag-valve-mask ventilation in a paediatric model.20 Two-person bag-valve-mask ventilation provided greater mean tidal volumes and peak pressures in the infant and child manikin models compared with the one-person technique. The two-person technique generated higher mean peak pressures than the one-person technique (infant: 27.4 vs 22.0; child: 27.2 vs 21.8). Wilson et al studied a two-handed mask-hold technique with a two-point top and spider hold in a term newborn manikin. They reported no significant difference in mask leak among the groups, with a median leak of 9% (2%–51%) in the two-handed technique.21 In our study, the median VTe was lower in the two-person mask method (6.4 in one-person vs 4.7 in two-person mask method, p=0.13), and the effect of jaw-thrust and chin lift on airway obstruction needs to be further evaluated.
In a study of preterm infants at resuscitation using a preterm manikin and RFM, there was a wide variation of leak at the mask–face interphase during each resuscitation and between resuscitators.22 They highlighted the importance of correct size mask and RFM to accurately assess the face mask leak and VTe. The RFM has been demonstrated to be useful in recording flow and pressure measurements in premature infants and was associated with significantly less mask leak.23 A study by van Zanten et al randomised infants under 28 weeks’ gestation to a visible or non-visible RFM at resuscitation. Percentage leak (>60%) was 17.4 (7.2–33.3) in the visible RFM versus 13.6 (3.7–32.1) in the non-visible group.24 The per cent of inflations within the target range was 30%, which was comparable to our study. Our study strengthens the importance of RFM in recognition of mask leak, airway obstruction and monitoring EtCO2 at resuscitation of extreme preterm infants.
Hooper et al showed that EtCO2 values may indicate aeration of distal airways.2 Their data on extreme preterm infants at birth demonstrated time to achieve EtCO2 more than 10 mm Hg from birth was 92 s (46–150) and 51 s (27–91) from start of mask ventilation. They reported a significant relationship of tidal volume and EtCO2 (EtCO2 increasing 0.15% with each 1 mL/kg increase in tidal volume). Our study demonstrated the use of EtCO2 in the delivery suite and its value in guiding ventilation. There was association of lower EtCO2 in breaths associated with significant airway obstruction and mask leak.
In adult patients, effectiveness of two resuscitators in terms of greater mask pressures and tidal volumes has been reported and well established.13 Resuscitation in newborn infants seeks to correct bradycardia/asystole and hypoxia by providing adequate alveolar ventilation. Breath-by-breath variation in mask leak may result in underinflation to over inflation with the potential for barotrauma and/or volutrauma, particularly in preterm infants. The optimal mask technique to provide adequate ventilation in resuscitation of extreme preterm infants needs to be further evaluated and the incidence of airway obstruction and mask leak further studied with use of a two-person mask method.
Strengths
The strengths of our study are that it is a prospectively randomised trial with documented RFM data from the first breath provided with PPV. The study validates the feasibility of a two-person mask technique in extreme preterm infants’ resuscitation at birth. We were prospectively able to demonstrate significant airway obstruction and mask leak in the delivery suite.
Limitations
This is a pilot study and hence the numbers are small within a single centre. The definition of mask leak and airway obstruction is not validated, although we used a strict definition of >75% mask leak/obstruction.
Conclusion
Mask leak and airway obstruction are common in resuscitation of preterm infants at birth. The use of two-person mask ventilation could be an effective option for clinicians if mask ventilation is not effective with a one-person method. Further studies are needed to further evaluate efficacy and safety of the two-person mask ventilation method.
Data availability statement
All data relevant to the study are included in the article or uploaded as an online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by HREC2013/10/4.4(3831). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to acknowledge Ms Annabel Webb for her statistical analysis and Ms Merran Laver for her professional editing of the manuscript.
References
Footnotes
Contributors DS and MBT conceptualised the study. DS performed the study. MKH transformed the digital data to .csv file and performed the analysis. DS wrote the manuscript. MBT, MBH and NB critically appraised the manuscript. DS is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.