Article Text

Abstract
Objective Interventions improving parent satisfaction can reduce parent stress, may improve parent-infant bonding and infant outcomes. Our objective was to systematically review neonatal interventions relating to parents of infants of all gestations where an outcome was parent satisfaction.
Methods We searched the databases MEDLINE, EMBASE, PsychINFO, Cochrane Central Register of Controlled Trials, CINAHL, HMIC, Maternity and Infant Care between 1 January 1946 and 1 October 2017. Inclusion criteria were randomised controlled trials (RCT), cohort studies and other non-randomised studies if participants were parents of infants receiving neonatal care, interventions were implemented in neonatal units (of any care level) and ≥1 quantitative outcome of parent satisfaction was measured. Included studies were limited to the English language only. We extracted study characteristics, interventions, outcomes and parent involvement in intervention design. Included studies were not sufficiently homogenous to enable quantitative synthesis. We assessed quality with the Cochrane Collaboration risk of bias tool (randomised) and the ROBINS-I tool (Risk Of Bias In Non-randomised Studies - of Interventions) (non-randomised studies).
Results We identified 32 studies with satisfaction measures from over 2800 parents and grouped interventions into 5 themes. Most studies were non-randomised involving preterm infants. Parent satisfaction was measured by 334 different questions in 29 questionnaires (only 6/29 fully validated). 18/32 studies reported higher parent satisfaction in the intervention group. The intervention theme with most studies reporting higher satisfaction was parent involvement (10/14). Five (5/32) studies reported involving parents in intervention design. All studies had high risk of bias.
Conclusions Many interventions, commonly relating to parent involvement, are reported to improve parent satisfaction. Inconsistency in satisfaction measurements and high risk of bias makes this low-quality evidence. Standardised, validated parent satisfaction measures are needed, as well as higher quality trials of parent experience involving parents in intervention design.
PROSPERO registration number CRD42017072388.
- neonatology
- outcomes research
- patient perspective
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Neonatal care significantly affects parents’ mental health; parent satisfaction is increasingly being used as a parent experience measure.
Parent satisfaction is inversely related to parent stress; interventions improving parent satisfaction have the potential to reduce parent stress, improve parent-infant bonding and infant outcomes.
Use of interventions measuring parent satisfaction as an outcome in neonatal units is increasing, although few are formally evaluated and wider uptake is limited; it is not known the degree to which parents are involved in intervention design.
What this study adds?
There is inconsistency in how parent satisfaction in neonatal care is defined and measured, and the majority of studies do not include parents in intervention design.
There is low-quality evidence that interventions relating to parent involvement may improve parent satisfaction with neonatal care.
Standardised, validated measures of parent satisfaction and higher quality trials, involving parents in intervention design, are needed.
Introduction
One in 10 newborn babies in high-income countries require neonatal care.1 This is stressful for parents, who often develop anxiety, depression and post-traumatic stress disorder symptoms.2–4 Parental stress interferes with parent-child bonding5 and there is a well-established link between maternal mental health and infant development.6 Parent satisfaction, defined as ‘the perception of parents’ needs and expectations being met’ is inversely related to parental stress.7 As such, it is increasingly being used as a parent experience measure and neonatal service quality indicator. Interventions aimed at improving parent satisfaction have the potential to reduce parent stress, improve parent-infant bonding8 and infant outcomes.9
A range of parent-centred interventions, such as including parents on ward rounds, have recently become widespread in neonatal practice. Many are implemented on a small scale, without evaluating their impact on parent experience, making long-term integration into neonatal services challenging, while many others are using parent questionnaires. ‘Parent satisfaction’ as an outcome is gaining momentum, as neonatal trusts attempt to match more ‘business-like models’ where effectiveness of interventions (and evidence for change) is measured by quantitative outcomes. Moreover, where parent experience is measured as ‘parent satisfaction’, some studies include it as a primary outcome, whereas others use it as a secondary indicator to explore the parent point of view.
Furthermore, there are multiple experience measures available in addition to parent satisfaction, including parent stress, anxiety and depression scales; both quantitative and qualitative. Finally, it is not known the degree to which parents are involved in the design of such interventions. There have been no previous systematic evaluations focused on interventions measuring parent satisfaction with neonatal care as an outcome.
The aim of this review is to identify and describe neonatal interventions relating to parents of infants of all gestations where an outcome was parent satisfaction. For the reasons outlined above, we have only included studies that reported ≥1 quantitative measure of parent satisfaction. We aim to report each intervention’s effect on parent satisfaction, as well as parent input in intervention design.
Methods
We reported this study using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.10 11 We searched MEDLINE, EMBASE, PsychINFO, Cochrane Central Register of Controlled Trials, CINAHL, HMIC, Maternity and Infant Care (online supplementary file 1) for English papers published between 1 January 1946 and 1 October 2017, with update searches on 1 September 2018.
Supplemental material
Inclusion criteria were: randomised controlled trials (RCT) and non-randomised studies (non-RCT) if participants were parents of infants receiving neonatal care, interventions were implemented in neonatal units and ≥1 quantitative outcome of parent satisfaction was measured. We have restricted our review to studies where ≥1 quantitative outcome of parent satisfaction was measured, in order to enable comparison of interventions, which has previously not been possible in any published review. Including studies with all available measures of parent experience (in addition to parent satisfaction), as well as those only qualitatively evaluated, would make any comparison very difficult. By using these preregistered search criteria, we also ensured we would capture studies measuring parent satisfaction both as primary and as secondary outcomes. We included studies from all neonatal care level units and all healthcare settings, without excluding studies in low-income or middle-income settings. This was because definitions of neonatal care levels differ between different countries and healthcare settings, making them not easily comparable. Moreover, different levels of care are found within the same hospital settings. We excluded systematic reviews, entirely qualitative studies, grey literature (eg, conference abstracts), studies only reporting protocols or abstracts and full reports not in English.
Two authors (SS, IA) independently double-screened titles and abstracts, reviewed full texts for eligibility and resolved any discrepancies with a third reviewer (JW). We extracted data using a pilot-tested, standardised data extraction form including study characteristics, interventions, outcomes and parent input into interventions’ design. We assessed methodological quality with the Cochrane Collaboration risk of bias tool12 for RCT and the ROBINS-I tool (Risk Of Bias In Non-randomised Studies - of Interventions)13 for non-RCT.
We presented individual study aggregate data in a narrative synthesis, grouped studies into themes using a Grounded Theory Approach14 and planned meta-analysis where data were appropriate for quantitative synthesis.
Patient and public involvement
This review was conceived in response to the clinical need identified by parents with neonatal care experience; a partnership including families with experience of preterm birth identified ‘what emotional and practical support improves attachment and bonding, and does the provision of such support improve outcomes for premature babies and their families?’ as a top 10 research priority.15 Additionally, this review was conceived as part of planning a wider project to pilot a neonatal intervention, with parents’ full input.16 Patients were not directly involved in the design, conduct, reporting or dissemination plans of our research.
Results
We identified 8362 studies for screening and assessed 73 full-text articles for eligibility (figure 1). A total of 32 studies describing interventions that measured parent satisfaction in neonatal care as an outcome met the inclusion criteria, reporting data from over 2866 parents, 1 study did not report number of parents. Our analysis included 10 RCT and 22 non-RCT: 3 cohort trials, 18 unspecified designs and 1 implementation project (tables 1–3). We further classified the unspecified non-RCT into two types, depending on how they defined their control groups and how they evaluated parent satisfaction (table 3).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of selected studies.
Included randomised controlled trials (RCTs)
Included prospective cohort studies
Included ‘other’ non-randomised controlled trials (non-RCT)
‘Unit-level effect’: studies that assessed parent satisfaction during a period of routine care (control group) and introduced the intervention at a later time, with a different group of parents. In these studies, improvement in parent satisfaction was evaluated between different parent groups, on a unit level.
‘Group level effect’: studies that formed intervention and control groups using convenience sampling during the same time period. Both groups (or sometimes only the intervention group) had satisfaction measured after the intervention period (postintervention testing). Baseline parent satisfaction was also measured in both groups (preintervention testing) in some studies. Improvement in parent satisfaction was demonstrated either by comparing outcomes between intervention/control groups following the intervention, or in comparison with the preintervention data.
Parent participants included mothers (14 studies), mothers and fathers (10 studies) or were not specified (7 studies). One study defined parent participants as a dyad of the mother with her designated support person. Median parent sample size was 63, ranging 7–482. This was higher for RCT (108 studies) compared with non-RCT (61 studies).
Study participants included parents of babies across the full range of gestations (23–42 weeks). Overall, 24/32 (75%) of studies involved preterm infants, 5/32 (16%) term infants and 7 studies did not state the gestational age of infants involved. Most studies (19, 59%) involved only preterm infants (up to 37 weeks); only one study (3%) involved only term infants and five studies (16%) involved both preterm and term infants. Preterm infants were included in 44% of RCT vs 63% of non-RCT.
Most studies were reported as conducted in level III neonatal units (17 studies), followed by level not stated (9 studies), level II–III (3 studies), level II (2 studies) and level I (1 study). Definitions of neonatal levels of care are not standardised but vary across different countries; none of the included studies have explicitly stated which definition applies to them.
Tables 1–3 show the key characteristics of included studies. They include a description of each study’s parent and infant sample, study design and intervention, outcome measures (timing and methods), results, parent input into intervention design and study impact on parent satisfaction.
Parent satisfaction
Outcome measures
All 32 studies reported they measured parent satisfaction as an a priori outcome. Only one study confirmed this through a protocol. Overall, 18/32 (56%) of studies (4/10, 40% RCT and 14/22, 64% non-RCT) reported a higher level of parent satisfaction associated with the intervention studied. Multiple different outcome measures within the domain of parent satisfaction were used; we grouped these into four categories: i) parent satisfaction (no additional description); ii) parent satisfaction with NICU care; iii) parent satisfaction related to specific components such as communication, staff or information; iv) parent satisfaction with a specific intervention.
Timing of measurement
Parent satisfaction was mostly measured ‘during infant admission only’ (24 studies; between 1 and 4 times), followed by ‘after infant discharge only’ (5 studies; 1 time) and ‘both during admission and after discharge’ (3 studies; between 1 and 3 times). In the majority of studies (19/32, 59%), no preintervention parent satisfaction measurements were conducted in the same parent groups with available postintervention data (ie, paired parent data for satisfaction levels did not exist). Instead, impact of interventions was determined comparing intervention/control group measurements in different time periods (tables 1–3).
Method of measurement
Parent satisfaction was assessed using 32 different methods: 29 different questionnaires, 2 different single questions and by structured interview in 1 study; in total, 334 different questions were used to assess parent satisfaction. Only 6/29 (21%) of questionnaires were reported to be fully validated (both content validation and reliability testing); 23/29 (79%) questionnaires were partially or completely unvalidated. The most commonly used questionnaire was the validated Neonatal Index of Parent Satisfaction17 questionnaire (three studies).
Interventions and impact on parent satisfaction
We grouped included studies into five intervention themes: parent involvement (14 studies); information provision/communication (8 studies); clinical care (7 studies); parent emotional support (2 studies); other (1 study). Parent involvement interventions were more commonly assessed in RCT compared with non-RCT .
We categorised interventions as effective or not effective based on whether a statistically significant difference between intervention and control groups was reported for parent satisfaction (boxes 1 and 2). None of the studies reported statistically significantly lower parent satisfaction in the intervention group compared with the control group. We classified studies as unclear if effective if they included small sample numbers or if statistical analysis was not performed (box 3). Finally, we highlighted studies where only the intervention group was assessed and only postintervention, where comparison to a control group was not possible (box 4).
‘Effective’ interventions in themes
Theme: parent involvement
More NICU access, parents on WRs, education (De Bernardo et al, Italy, 2017)
Rooming-in care (Kazemian et al, Iran, 2016)
Parental presence at clinical bedside rounds (Abdel-Latif et al, Australia, 2015) RCT
More NICU access, care involvement, education (Bastani et al, Iran, 2015) RCT
Education regarding pain management (Franck et al, UK, 2011) RCT
Single-family NICU rooms (Stevens et al, USA, 2011)
Family centered rounds (Voos et al, USA, 2011)
Newborn Individualised Developmental Care and Assessment Programme (Wielenga et al, The Netherlands, 2006)
Infant progress charts filled by parents and three care planning meetings (Penticuff and Arheart, USA, 2005)
Kangaroo care (Legault and Goulet, Canada, 1995)
Theme: information provision / communication
Internet-based education (Kadivar et al, Iran, 2017)
Daily SMS from electronic patient record (Globus et al, Israel, 2016)
Staff education, staff contact card given to parents, staff poster at NICU reception (Weiss et al, USA, 2010)
Provision of taped conversations with neonatologists to mothers (Koh et al, Australia, 2007) RCT
Theme: clinical care
Headbox oxygen for respiratory distress
Continuous oxygen positive airway pressure for respiratory distress (Foster et al, Australia, 2008)
Co-bedding infants in incubators (prospective) (Byers et al, USA, 2003)
Co-bedding infants in incubators (retrospective) (Polizzi et al, USA, 2003)
Theme: parent emotional support
Narrative writing (Kadivar et al, Iran, 2017)
Interventions where parent satisfaction was reported to be statistically significantly higher in the intervention group.
NICU, neonatal intensive care unit; RCT, randomised controlled trial; WR, ward round
‘Ineffective’ interventions in themes
Theme: parent involvement
Massage with auditory, tactile, visual and vestibular stimulation
Kangaroo care (Holditch-Davis et al, USA, 2013) RCT
Individualised, developmentally supportive family centred care interventions (Byers et al, USA, 2006)
Theme: information provision/communication
Sharing information obtained from parent interviews with the primary NICU provider (Clarke-Pounder et al, USA, 2015) RCT
Theme: clinical care
Clinical nurse specialist/neonatal practitioner team care (Mitchell-DiCenso et al, Canada, 1996) RCT
Theme: other
Free parking (Northrup et al, USA, 2016) RCT
Interventions where parent satisfaction was not reported to be statistically significantly different in the intervention group.
RCT, randomised controlled trial.
‘Unclear if effective’ interventions in themes
Theme: parent involvement
Open unit policy: 24/7 NICU access (Voos and Park, USA, 2014)
Touch and massage for 7 days (Livingston et al, USA, 2009) RCT
Theme: information provision/communication
Clinical staff enter updates in baby diary (Van de Vijver and Evans, UK, 2015)
Detailed information provided during consenting (Broyles et al, USA, 1992) RCT
Theme: clinical care
Palliative care (Petteys et al, USA, 2015)
Five potentially better practices in the area of discharge planning (Mills et al, USA, 2006)
Interventions where small study numbers and/or no statistical analysis performed).
RCT, randomised controlled trial.
Interventions in themes where ‘only the intervention group was assessed and only postintervention’
Theme: information provision/communication
Daily parent update letter from electronic patient record (Palma et al, USA, 2012)
Theme: clinical care
Tele-rounding robot, off-site neonatologist (Garingo et al, USA, 2016)
Theme: parent emotional support
Listening visits (Segre et al, USA, 2013)
Overall, 18/32 studies (56%) reported higher parent satisfaction in the intervention group; 4/10 RCT and 14/22 non-RCT. The intervention theme where higher satisfaction was most consistently reported was parent involvement (10/14 studies). Due to the large heterogeneity of outcome measure scales, a quantitative synthesis and meta-analysis was not possible.
Parent input into design of interventions
Five studies (5/32, 16%) reported involving parents in intervention design, of which two reported improvement of parent satisfaction. The number of included studies was too small to estimate any effect of parent co-design on the success of interventions at study level.
Methodological quality
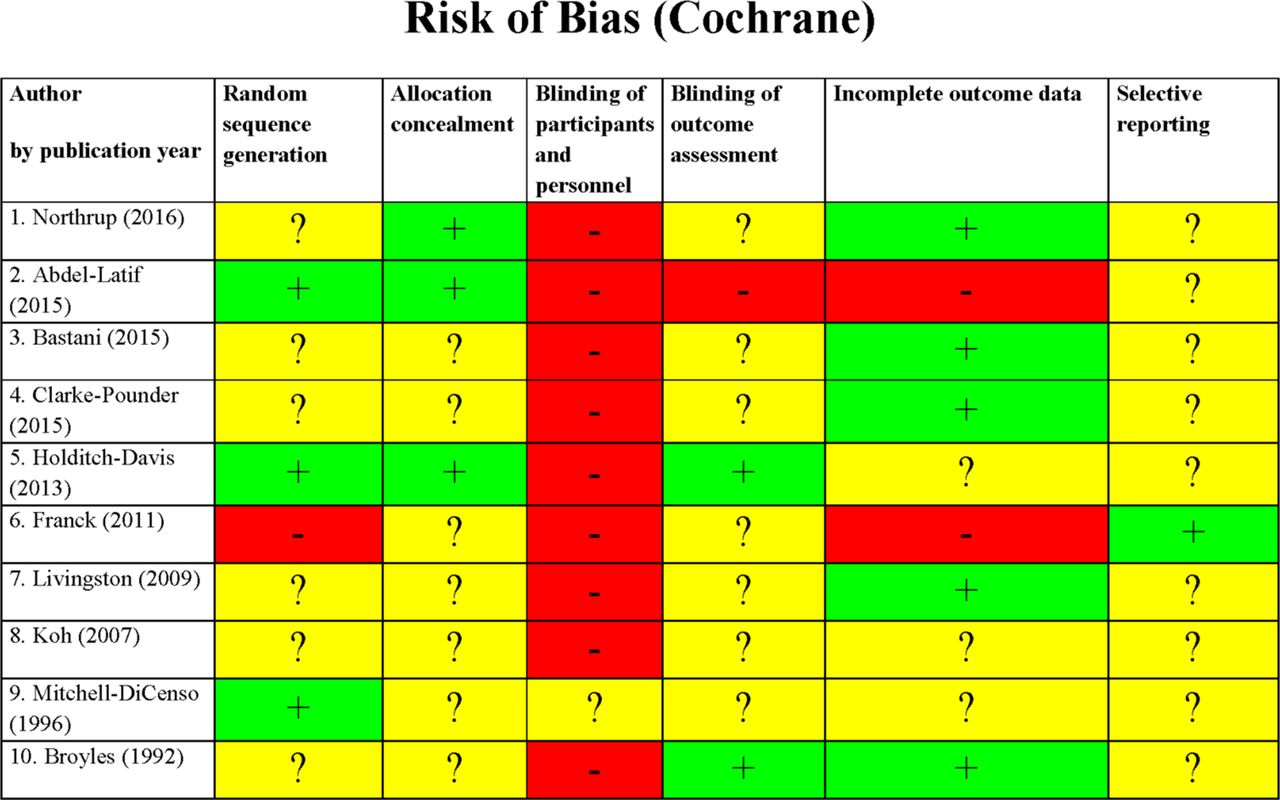
For the majority of RCT, key study characteristics, such as randomisation, allocation concealment and blinding of outcome assessment, were either not stated or unclear (figure 2). Only one RCT had an available study protocol (retrospectively registered) and none described blinding of study participants and/or personnel. All RCT scored a high/unclear risk of bias in at least 4/6 Cochrane tool categories, except for one, which scored a high/unclear risk in 3/6 categories.

Cochrane Collaboration risk of bias tool assessment (randomised controlled trial). Green: low risk of bias; yellow: unclear risk of bias; red: high risk of bias.
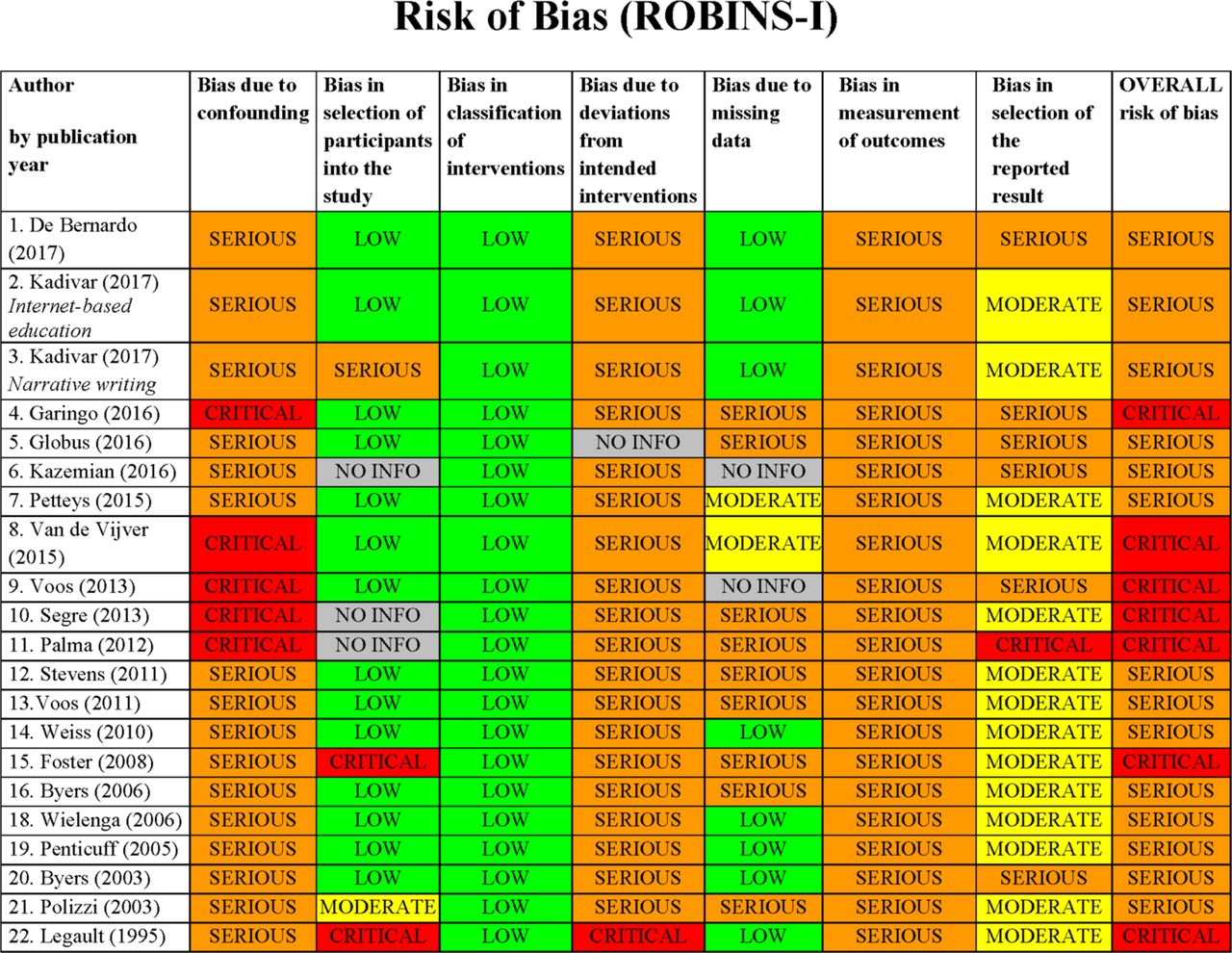
We assessed 21/22 non-RCT studies using the ROBINS-I tool13, excluding the implementation project. All 21 studies were assessed as having an overall serious risk of bias and 7/21 of studies (33%) were further categorised as having critical risk of bias (figure 3). Blinding of participants, personnel and outcome assessment was poorly reported across all non-RCT and no study reported a published study protocol. None of the included non-RCT measured or corrected for important parent/infant confounding variables, or other relevant neonatal unit co-interventions taking place at the same time as the intervention.
{kind=link}
{kind=link}
{kind=link}
ROBINS-I risk of bias assessment (non-randomised controlled trial).
We were unable to use the Standards for Reporting Implementation Studies (StaRI) Statement Tool18 for assessing the implementation project, as the reporting was incomplete.
There was no association between methodological quality assessments and the studies’ reported effect on parent satisfaction. All 4/10 RCT that reported a higher level of parent satisfaction associated with their intervention, scored a high/unclear risk of bias in at least 4/6 Cochrane tool categories, one of which scored high/unclear risk in all categories. Out of the 14/22 non-RCT reporting an improved parent satisfaction, two were deemed to be at critical risk of bias on the ROBINS- I tool, while the rest we assessed to be at serious risk of bias.
Discussion
Parent satisfaction with neonatal care is increasingly recognised as an important measure of parent experience and is being used to evaluate hospitals and healthcare providers; use of interventions to improve parent satisfaction in neonatal units is increasing. This is the largest review of interventions where an outcome was parent satisfaction with neonatal care and includes 32 studies. We find low-quality evidence that interventions targeting ‘parent involvement’ may improve parent satisfaction with neonatal care, but this result must be interpreted cautiously in view of the high risk of bias in included studies.
Overall, our review highlights the complexity of evaluating parent satisfaction. As a multidimensional construct, parent satisfaction can be affected just as much by interventions directly relating to infant care (eg, Kangaroo care) as well as interventions relating to neonatal care facilities (eg, Free parking). By grouping included interventions into themes (boxes 1–4), we have highlighted the variety of interventions available, as well as the majority of interventions being those relating to ‘parent involvement’.
A key reason for only selecting parent satisfaction as the outcome of interest was to focus on a single component of parent experience, in order to reduce outcome heterogeneity and allow direct comparison. Despite this approach, the key methodological limitation identified in this review was inconsistency in how parent satisfaction is defined and measured; it is notable that the majority of questionnaires (23/29) lack validation. In keeping with neonatal studies more widely,19 this study confirms inconsistent outcome selection as a major source of research waste in neonatal studies examining parent experience, and further finds that there is limited involvement of parents in study design.
Strengths of our review include identifying studies with both mother and father participants, inclusion of the full range of infant gestations and a wide range of interventions. We followed a preregistered protocol and report this review in line with PRISMA guidelines.11 To further aid direct comparison of interventions, we only included studies that evaluated parent experience using ≥1 quantitative outcome of parent satisfaction. One limitation of this approach is that by excluding studies which evaluated parent experience using other measures (eg, stress, anxiety and depression scales), we are unable to comment on interventions that targeted these other components of parent experience.
Another limitation is that we have only included studies in the English language, due to resource and time constraints. By not including studies in other languages, it is possible our results are more focused on work conducted in specific countries. Furthermore, we acknowledge that much of the research in parent experience is qualitatively evaluated. By restricting our review to studies where ≥1 quantitative outcome of parent satisfaction is measured, we have not included any interventions with solely qualitative outcomes. This was in an attempt to enable direct comparison of interventions, which has previously not been possible in any published review. By not including studies evaluated by qualitative measures only, it is possible our results are more focused on a particular type of interventions where quantitative evaluation would be preferable and/or easier. It also means we may not have included all studies ever conducted on a particular intervention, where some were only evaluated qualitatively, making some interventions appear more ‘widespread’ than others.
Brett et al20 systematically reviewed interventions aimed at improving the parent experience more widely, but only included parents of preterm infants. Their large number of outcome domains and heterogeneity of outcome measures (including studies that reported only qualitative outcomes) meant the authors we unable to draw firm conclusions about the efficacy of interventions and that comparison and meta-analysis was not possible. The majority of our review’s studies have been published in the 7 years since the review by Brett et al, highlighting the increasing interest in this area. However, despite including all gestations and focusing on a specific aspect of parent experience, heterogeneity in measurement of parent satisfaction meant we were also unable to conduct a quantitative synthesis. Inconsistency and lack of validation of instruments measuring parent satisfaction in neonatal care (specifically with family centred care) has also previously been highlighted by Dall’Oglio et al.21
Although 31% of included studies were RCT, all were assessed as having a high risk of bias. RCTs are traditionally considered the highest-ranking form of evidence, however it is worth considering whether such a design is feasible or desirable to evaluate interventions targeting parent satisfaction. Parents in neonatal care talk to each other, compare notes and invariably create parent-support communities; hence it is inherently difficult to avoid contamination between parents receiving an intervention and those who are not, meaning that blinding of parents or health professionals is near impossible. Furthermore, parent satisfaction is likely to be particularly susceptible to the Hawthorne effect,22 requiring longer-term follow-up. These factors may explain the low number of RCT identified in our review and the high risk of bias seen in those that were included. In non-RCT studies, the main methodological concern is the degree to which unmeasured and uncontrolled confounders may explain any differences seen between groups. The non-RCT studies included in this review were classed as having either a serious or critical risk of bias. The overwhelming majority of studies did not adequately report baseline variables or report other interventions during the study period, making it impossible to assess studies for selection bias or treatment bias. Furthermore, limitations such as contamination bias and the Hawthorne effect affect non-RCT as well. Only two non-RCT studies evaluated the outcome of interest (parent satisfaction) both before and after the intervention, in the same group of parents (group level effect), with most studies evaluating different parent groups preintervention and postintervention (unit level effect). An inherent weakness of this latter approach is that it assumes parent satisfaction is a static measure at the unit level, which is unlikely to be true. As a result of these numerous important limitations identified across all included studies, we find only low-quality evidence in support of interventions to improve parent satisfaction with neonatal care, despite a majority of studies reporting a beneficial effect of interventions. These limitations may explain the limited uptake of these interventions by the wider neonatal community.
Changing neonatal unit practices to incorporate any new intervention requires robust evidence. We demonstrate here that such evidence is not currently available for improving parent satisfaction. We highlight the use of non-randomised study designs, inconsistency in definition and measurement of parent satisfaction, the use of unvalidated questionnaires, methodological limitations and a lack of parent involvement as contributors. Our review empirically documents the extent of these issues in studies that use quantitative parent satisfaction surveys, and their contribution to research waste in neonatology.
Given the importance of parent satisfaction for both parent and offspring well-being, higher quality trials that involve parents, use of standardised definitions and validated parent satisfaction measures are needed. Given the nature and challenges of the neonatal care environment and the limitations we have identified in existing research, a cluster RCT may be the most appropriate study design to rigorously evaluate interventions to improve parent satisfaction with neonatal care.
Conclusions
Many interventions, commonly relating to parent involvement, are reported to improve parent satisfaction with neonatal care but inconsistency in definition and measurement of parent satisfaction and high risk of bias in all studies makes this low-quality evidence. Standardised definitions and validated parent satisfaction measures are needed, as well as higher quality trials of parent experience, involving parents in intervention design.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
References
Footnotes
Twitter @DrCGale
Correction notice This article has been corrected since it was first published. Provenance and peer review statement has been corrected.
Contributors SS and CG conceived this systematic review. The protocol was created by SS and CG. Searches were performed by SS and IA. All search results were reviewed by SS and JW. Coding was completed by SS and JW. Data analysis was completed by SS. The first draft of the manuscript was written by SS; SS, CG and JW edited and reviewed the manuscript. All authors approved the manuscript. This article presents independent research supported by the National Institute for Health Research (NIHR).
Funding This work is sponsored by Imperial College London and supported by a peer-reviewed National Institute of Health Research Doctoral Research Fellowship, awarded to SS (DRF-2017-10-172).
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Competing interests SS has received research grants from the National Institute of Health Research (NIHR), the NIHR CLAHRC NWL, Rosetrees Trust and CW+ charity. NM is Director of the Neonatal Data Analysis Unit at Imperial College London. In the last 5 years, NM has served on the Board of Trustees of the Royal College of Paediatrics and Child Health, David Harvey Trust, Medical Women’s Federation and Medact; and is a member of the Nestle Scientific Advisory Board. NM has received research grants from the British Heart Foundation, Medical Research Council, National Institute of Health Research, Westminster Research Fund, Collaboration for Leadership in Applied Health and Care Northwest London, Healthcare Quality Improvement Partnership, Bliss, Prolacta Life Sciences, Chiesi, Shire and HCA International; travel and accommodation expenses from Nutricia, Prolacta, Nestle and Chiesi; honoraria from Ferring Pharmaceuticals and Alexion Pharmaceuticals for contributions to expert advisory boards and Chiesi for contributing to a lecture programme. CG is funded by the UK Medical Research Council (MRC) through a Clinician Scientist Fellowship award. He has received support from Chiesi Pharmaceuticals to attend an educational conference; in the past 5 years, he has been investigator on received research grants from Medical Research Council, National Institute of Health Research, Canadian Institute of Health Research, Department of Health in England, Mason Medical Research Foundation, Westminster Medical School Research Trust and Chiesi Pharmaceuticals.
Provenance and peer review Not commissioned; externally peer reviewed.