Article Text

Abstract
Background Paediatric mental health patients frequently use natural health products (NHP) in addition to prescription medications, but very little is known about adverse events and possible NHP–drug interactions.
Objective To determine: (1) the prevalence of paediatric mental health patients taking prescription medications only, NHP only, both NHP and prescription medications concurrently or neither; (2) which prescription medications and NHP are most commonly used in paediatric mental health populations and (3) adverse events experienced in the last 30 days (serious and non-serious).
Design Cross-sectional surveillance study.
Setting Paediatric mental health clinics.
Population/intervention On their first clinic visit, paediatric mental health patients were provided with a form inquiring about prescription drug use, NHP use and any undesirable event experienced in the last month.
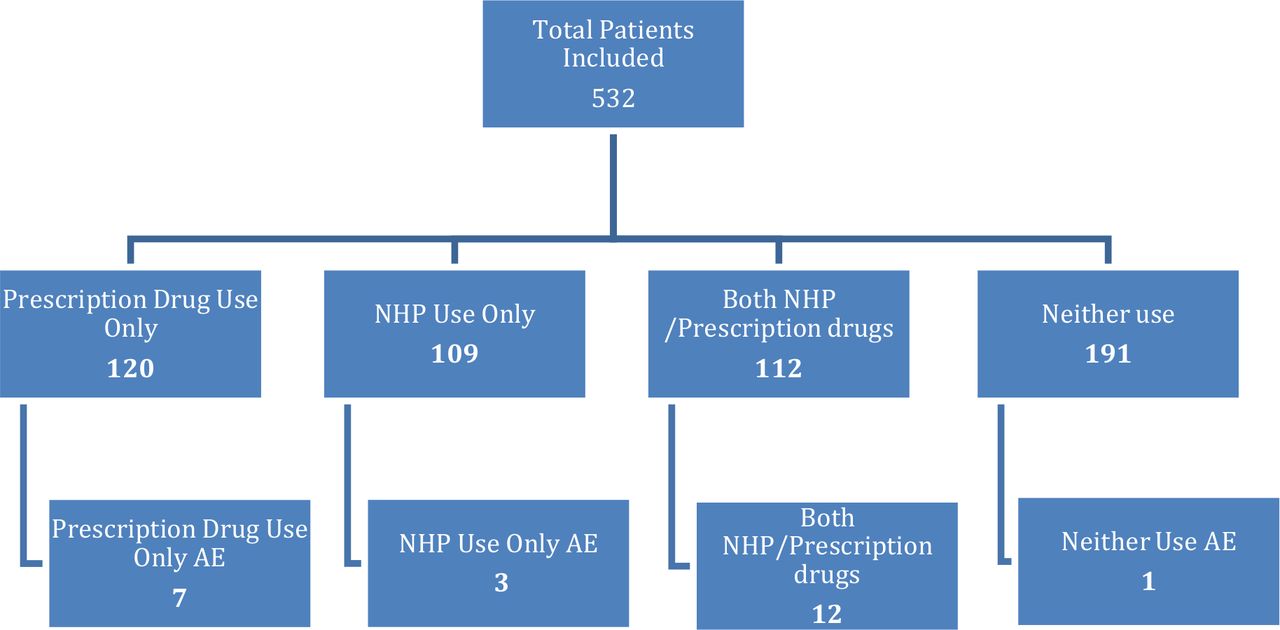
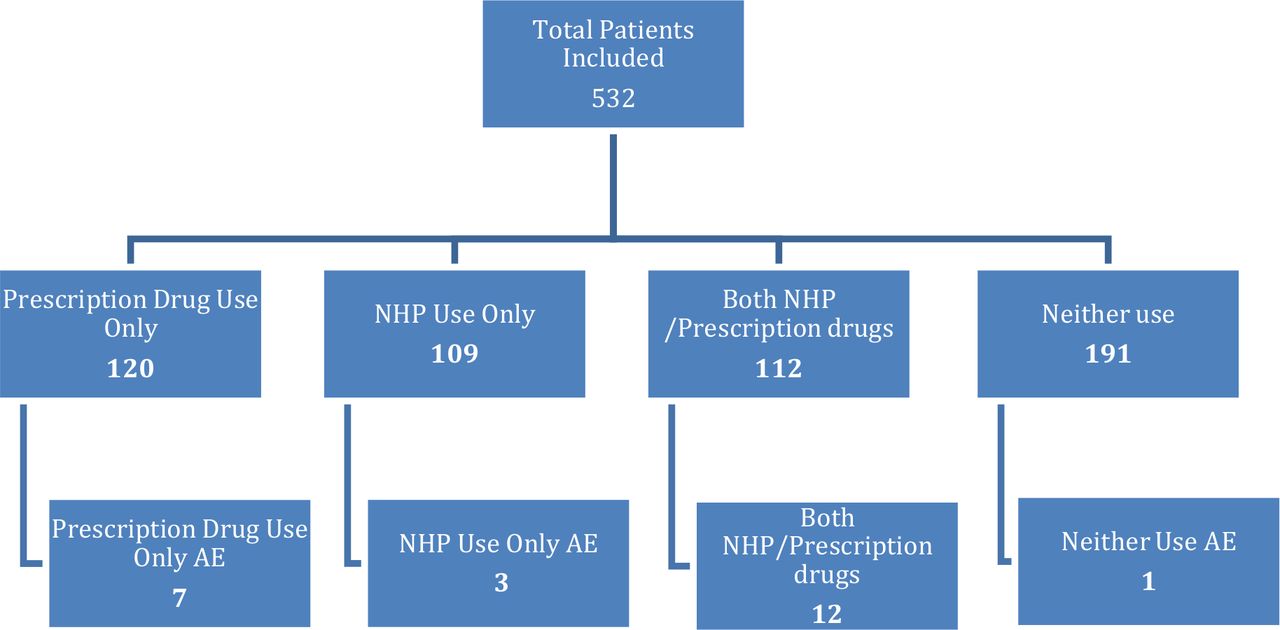
Results Of the 536 patients included in this study, 23% (n=120) reported taking only prescription medication(s), 21% (n=109) reported only NHP use, 21% (n=112) reported using both NHP and prescription drugs concurrently, and 36% (n=191) reported using neither. Overall, there were 23 adverse events reported; this represents 6.3%, 2.8%, 10.8% and 0.6% of each population, respectively. The majority of patients who experienced an adverse event reported taking more than one NHP or prescription drug. No serious adverse events were reported.
Conclusion Nearly half of the paediatric mental health patients in this study were taking NHPs alone or in addition to prescription medications. Active surveillance identified multiple adverse events associated with NHP and prescription drug use; none were serious. Healthcare professionals were encouraged to initiate conversations regarding NHP use.
- alternative medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Paediatric mental health conditions are highly prevalent worldwide.
Patients with chronic conditions often use natural health products.
Polypharmacy use increased the number to adverse events experienced by the patient.
Active surveillance of adverse events is more reliable method of pharmacovigilance if compared with passive methods.
What this study adds?
Children with mental health conditions take natural health products in addition to prescription medications.
Active surveillance demonstrated to be feasible in the clinical setting.
Introduction
Paediatric mental health conditions are highly prevalent worldwide. In Canada and USA, it is estimated that between 15% and 25% of youth experience at least one mental health disorder.1 2
In France, a cohort study found 6.3% of 17-year-old girls were prescribed a psychotropic drugs (anxiolytic, antidepressant or hypnotic).3 In Iceland, a population survey found that 4.9% of children and adolescents were in use of a psychotropic drug.4
Natural health products (NHPs) are commonly used in patients with serious, chronic or recurrent illness, including patients with mental health conditions.2 A recent study found that 56.3% of paediatric patients with chronic health problems were taking NHPs in addition to conventional therapy.5 Two adult cross-sectional studies done in patients with mental health conditions found 25% –66% of patients use at least one NHP and often in association with prescription drugs (29.7%–58%).6 7 The high prevalence of NHP use in patients with mental health disorders may be attributed to factors like easier accessibility than prescription medications, dissatisfaction with conventional medications and the perceived ‘naturalness’ of NHPs.7 8 Many patients assume that because a product is ‘natural’, it is safe, and will have fewer side effects.9 In Canada, NHPs are regulated by Health Canada and include vitamins and minerals, herbal medicines, homeopathic remedies, traditional Chinese medicine, probiotics, amino acids and essential fatty acids.10 NHPs used to support mental health include valerian, kava, ginko and St. John’s wort, which interact with commonly used medications.11 12 For example, the use of selective serotonin reuptake inhibitors with St. John’s wort could result in serotonin syndrome.13
The risk of interactions and adverse events (AEs) increases with the number of products taken.14 In a population survey, the incidence of potentially serious drug–drug interaction was directly associated with the number of drugs dispensed: 10.9% if dispensed 2–4 drugs vs 80.8% if dispensed ≥15 drugs.15 Recently, it was found that adult patients with mental health disorders taking prescription and NHP concurrently are 2.8 times more likely to experience an AE than patients taking prescription medications alone.16 To date, there are no data on the risk of NHP–drug interactions and AEs among children with mental health disorders.
We undertook a cross-sectional surveillance study to investigate the AEs associated with concurrent NHP and prescription drug use in paediatric mental health patients. The objectives of this study were to determine: (1) the prevalence of paediatric mental health patients taking prescription medications only, NHPs only, NHPs and prescription medications concurrently or neither; (2) which prescription medications and NHPs are most commonly used in paediatric mental health populations and (3) AEs experienced in the last 30 days (serious and non-serious).
Methods
We followed the Strengthening the Reporting of Observational Studies in Epidemiology guideline to report this observational study.17 Patients and the public were not involved in the development of methods, analysis or dissemination of this study.
Eight paediatric mental health clinics in Alberta were invited to participate in this project. Each clinic was provided with initial on-site training in the relevance of the projects and how to use the screening forms, in addition, follow-up meetings and ongoing phone, email and on site contact were provided by the research group throughout the study period to support clinics and answer any possible questions. All required resources, digital and hard copy screening logs for printing and distribution, training presentations and definitions of NHP and drugs were provided to participating clinics.
NHPs are defined by Health Canada as a substance which includes vitamins and minerals, herbal medicines, homeopathic remedies, traditional medicines (eg, traditional Chinese medicine), probiotics, amino acids and essential fatty acids as at least one of its medicinal ingredients.10 We followed Health Canada’s classification for an NHP, whether or not the NHP was prescribed. For example, oral iron supplementation was classified as a NHP as this is how it is classified by Health Canada, whether or not it was prescribed by a health professional.10
A prescription drug was defined as any drug prescribed by a healthcare professional or an over-the-counter (OTC) drug with a drug identification number.
AE was defined as an unexpected or undesirable event, including reduced or lack of therapeutic effect as assessed by clinical opinion.16 18
A serious AE was defined as one that is: life-threatening, leads to initial or prolonged hospitalisation, leads to persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions, results in congenital anomaly/birth defect, causes death or an important medical event that could be considered serious when, based on medical judgement, may jeopardise the patient or require medical or surgical intervention.19
All patients/guardians of children up to 18 years old, receiving care from participating clinics were given a survey form on their first clinic visit, containing the following questions regarding their child’s prescription drug use, NHP use and AEs in the last month.
(Q1) In the last 1 month, has your child taken any prescription medications? If yes, list the medications and for how long have they been taken?
(Q2) In the last month, has your child taken any NHPs, for example, vitamins, minerals, herbals, homeopathic remedies, traditional Chinese medicines, probiotics? If yes, list the NHPs and for how long have they been taken.
(Q3A) In the last 1 month, has your child experienced any unexpected or undesirable side effects or symptoms? If yes, describe the effects.
(Q3B) What did you do about it?
(1) Nothing, (2) treated myself, (3) phoned for information, (4) saw a doctor about it, (5) doctor ordered tests, (6) doctor treated it or (7) my child was hospitalised.
The completed form was reviewed by the patient’s clinic healthcare professional (therapist, nurse, physician, etc), who would assess any AE reported by the patient and identify if, in their opinion, the event was ‘serious’; ‘unexpected’ and/or ‘caused a delay or change in treatment’.
The patient’s healthcare professional was also given the opportunity to report any other AE by answering the question:
(Q4) In the last month, has the patient had any other AEs? If yes, describe the event and investigation/treatment required. Please identify if: Serious, unexpected or caused a delay or change in treatment.
These screening questions were considered part of ‘best possible medication history (BPMH), as suggested by the Canadian Institute of Patient Safety, meaning that a systematic approach to interview patient or family should be undertaken in every clinic visit as part of best practice.20
In this study, AE seriousness was identified based on: (1) event reported, (2) the level of care sought by the participant to treat the AE and (3) the healthcare provider assessment of the event (if considered the event serious or not). If a potential serious AE was identified, the patient/guardian was asked if they would like to participate in a research study to learn more about the AE. If the patient or guardian consented, the study coordinator contacted the patient within 1 week. Via a phone interview, our team obtained verbal consent, and inquired about the patient’s health state and all products (prescription, OTC and NHPs) including brand and dose. If appropriate, we requested permission to obtain samples of the products via courier; these samples would then be shipped directly to participating laboratories for analysis of possible contaminants or adulterants. If a serious AE associated with a NHP occurred, it would be forwarded to Health Canada within 48 hours of identification for their review.
Data collection and data analysis
Study data were collected and managed using Research Electronic Data Capture tools hosted at University of Alberta.2 21
Results
Five mental health clinics participated in the study. A total of 539 patients were each screened once between 2014 and June 2018. Seven incomplete surveys were excluded from analysis (one did not provide information about prescription drug use; one did not provide information about NHP use; four had unspecified locations and therefore could not be weighted appropriately; one reported an AE, but did not report if patient was taking NHP or prescription drugs). Of the 532 included patients, 229 reported diagnostic information with the most common being anxiety (n=83) and attention-deficit/hyperactivity disorder (n=77). More detailed information about the study population can be found in table 1.
Characteristics of study population
Adverse events
A total of 492 of 532 (92.5%) forms provided complete AE information to be included in the analysis. Overall, 4.7% (n=23) of patients with complete AE data reported an adverse event. More details on the adverse events reported in each category are found in figure 1. Table 2 provides more details of all 23 AEs identified.
{kind=link}
NHP and prescription drugs use and related AEs. AEs, adverse events; NHP, natural health product.
Summary information for reported AEs for patients taking Rx meds and/or NHPs
The number of AEs increased proportionally with the number of products taken. Of the patients taking three prescription medications, 28.6% experienced an AE. More than 70% of patients who experienced an AE were taking more than one product (NHP or drug).
The AEs reported ranged from migraines, to suicidal ideation, however, the most common AEs were fatigue (18.3%) and decreased appetite (18.3%). No serious AEs were reported. One patient reported suicidal ideation was not taking any NHP or prescription drugs, she/he was not hospitalised and the healthcare professional did not identify the event as serious, therefore, it did not fulfil the study criteria for seriousness.
The most common prescription medications taken were methylphenidate (n=32) and oral contraception (birth control pill) (n=24). The most common NHPs were multivitamins (n=101) and melatonin (n=82). The most common NHP–drug combinations taken were methylphenidate and melatonin (n=11) and methylphenidate and multivitamins (n=10).
Discussion
Mental health conditions are highly prevalent and generate a high healthcare cost, in the USA, for example, it is estimated at US$247 billion per year.1 22 Parents and patients often seek alternatives to prescription medications for management of mental health conditions. Many children and parents opt to use complementary therapies as adjunct treatment for mental health conditions because they are perceived as helpful and natural.7 Despite the frequency of NHP use in paediatric mental health conditions, there are no studies to our knowledge assessing NHP and drug-related AEs in this population.
We present a cross sectional active surveillance study of AEs associated with NHP and prescription drug use in paediatric patients with mental health conditions. Nearly half of patients included in the study were taking NHPs, alone or in association with a prescription medication. A majority of AEs identified was associated with the use of two or more products. Necyk et al found that 25.5% of adult mental health patients taking NHPs and drugs concurrently experienced an AE,16 however, adult mental health patients are more likely to be taking a higher dose and quantity of medications than paediatric patients, which increases the chances of AEs.23
Polypharmacy is well known to increase the risk of AEs in multiple populations. In a population-based study in Scotland over 15 years, the proportion of adults dispensed ≥5 drugs doubled, as a consequence the proportion of potentially serious drug–drug interactions more than doubled in the same period.15 Older outpatient adults taking five or more medications had an 88% increased risk of experiencing an adverse drug event compared with those who were taking fewer medications.24 Interaction was also a concern: in hospitalised adults taking five or more medications, the prevalence of a potential hepatic cytochrome enzyme-mediated drug-drug interaction was 80%.25 NHP and prescription drugs are often used in combination in children, but multiple studies have confirmed that NHP use is often not disclosed to the healthcare professional.26 27
Adults with mental health conditions are known to have high intake of NHP.16 28 In a study by Necyk et al, 19% of adult mental health patients reported using NHPs and prescription medications concurrently.16 We found a similar rate of concurrent use, suggesting that paediatric patients frequently take NHPs in association with prescription medications. The results of our study were consistent with similar studies involving concurrent drug and NHP use in mental health patients.5 7 16 29 In a recent study, Wang et al identified that American children with mental health disorders are more commonly using complementary treatments compared with those without (19.2% compared with 10.1%, p<0.001) and herbal medicines are the most frequently used modality.30
Study strengths
This study uses active surveillance to investigate NHP and drug AEs in paediatric mental health patients. Active surveillance ‘seeks to ascertain completely the number of AEs via a continuous preorganised process’ which appears to increase rates of reporting, produce better quality reports and encourage communication between patients and healthcare professionals regarding NHPs.9 Active surveillance has been used in the past to investigate NHP–drug AEs; however, to our knowledge, this is the first study to investigate in this population. Most countries, including Canada, use passive surveillance in detecting adverse events, which refers to voluntary reporting of an adverse event.31 Although passive surveillance has the capacity to identify rare AEs, under-reporting and poor-quality reports make this method less than ideal9 In a study by Zimmerman et al, active surveillance identified 1.65 AEs reports per every 100 paediatric patients, compared with the Canada Vigilance Programme which used passive surveillance and only identified 0.17 AEs in every 100 paediatric patients.32 Our active surveillance study identified 4.5 AEs per 100 paediatric patients with mental health conditions. Active surveillance has been found to increase AE reporting and we have demonstrated its feasibility in the clinical setting.16
This study identified that paediatric mental health patients are often using NHPs, with nearly half of included patients reporting NHP use. The Canadian Safety Institute recommends, as part of BPMH, that all product history should be obtained at every clinic visit; however, in practice NHP use and AE reporting are rarely captured16 Patients have reported that they believe that NHPs are ‘natural’ and therefore safe, suggesting that patients believe that healthcare professionals do not need to know about such use.9 In a study by Adams et al, only 20% of paediatric patients told either their physician or pharmacist that they were using complementary therapies concurrently with prescription medication.5 To compound this issue, when patients do tell healthcare professionals about NHP AEs, many do not report that AE to Health Canada. In one study by Charrois et al, only 1.5% of pharmacists reported NHP–drug interactions to Health Canada.9 Without adequate reporting, the safety of paediatric NHP use is uncertain.33 Our study stimulated discussion between patients and healthcare providers about NHP use and encouraged AE reporting through active surveillance. Discussing all therapies and their reasons for use promotes patient-centred care as well as patient safety. We hope this practice will remain after the study ends, as part of best practice.
Study weaknesses
A possible limitation of our study is that NHP/drug use and corresponding AEs were sought during the first clinic visit. While this simplifies analysis by ensuring data are independent, we feel patients should be asked about all products and all AEs at every visit.
Additionally, this study was limited to five mental health clinics within one geographical area (Alberta, Canada). Thus, our study may not represent NHP use in other settings; further work to investigate NHP use by paediatric mental health patients in different settings is needed and encouraged.
This study identified reported AEs and possible association with prescription drugs and NHP, although direct causation of the AE was not investigated. We are unable to differentiate whether patients with more symptoms take more medications, or if they take more medications and have more symptoms. While we had study methods to allow for more definitive assessment of AE, such as laboratory assessment, these resource-intensive methods were reserved for serious AE, which did not occur.
Future steps
BPMH advocates for collection of accurate information of all therapies taken by the patient, which should include prescription drugs and NHPs.20 There is also a need to expand the BPMH inquires to include any possible undesirable adverse effects caused by therapeutic products, increasing awareness of possible adverse effects to patients and healthcare professionals. Product-related adverse effects are responsible for multiple hospital admissions and the morbidity and mortality related to the AEs is directly associated to the number of drugs taken.34 35 Open discussion between patients and healthcare professionals regarding all therapies, including NHPs and associated AEs are key to fully understanding patient’s health. Promoting the discussion of NHP use is critical to to enhance patient safety and promote patient-centred care.36
Pharmacoepidemiological surveillance is a key element to improve patient safety outcomes. AEs are often rare. Information on AEs acquired on population level is feasible and reliable method to identity AEs, or lack thereof, which is also informative.
Any surveillance study does not have a primary goal to improve clinical outcomes. Surveillance studies identify safety signals. Once a signal is identified, it triggers further investigation to assess its definitive causality and clinical practice change as a further step. If AEs are not monitored, they are often not reported and neglected, but still present, ultimately injuring patients due its lack of investigation.
The probability of identifying and reporting an AE increases dramatically when using active surveillance.32 This study introduced active surveillance as a mechanism to help clinical staff become comfortable asking about NHP use, and shown itself to be feasible. The study has ended, but it appears participating healthcare professionals have incorporated questions about NHP use and product-related AEs as part of their routine patient history.
Continued research into the concurrent use of NHPs and prescription medications support the development of a database of which combinations have associated adverse effects and which do not, greatly enhancing current knowledge of clinically relevant NHP–drug interactions.
Conclusion
In this observational study of AEs in paediatric mental health patients, many patients were taking NHPs, alone or in combination with a prescription medication. Polypharmacy, including mixing NHPs and prescription medications, increases the likelihood of an AE; no serious AEs were identified in this study. Active surveillance has demonstrated it is feasible and should be considered as a preferred method of pharmacovigilance to enhance AE identification and reporting.
Acknowledgments
We would like to thank to all members of the SONAR steering committee for their contributions on the development of the SONAR projects. A special thank you to Dr. Heather Boon for her ongoing active collaboration in this work.
References
Footnotes
Twitter @bkhamba
Contributors ES, LZ, BK and CN collected and analyzed the data. JB, LU and SV developed the idea. LZ, BK, CN, JB, LU and SV implemented the project. ES, LZ, BK, CN, JB, LU and SV developed the manuscript and revised the final version submitted.
Funding This work was supported by a partnered grant form Canadian Institute of Health Research (CIHR) (#RES0021177) and Alberta Innovates Health Solutions (AIHS) (#RES0025318).
Competing interests None to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Approval by the Human Research and Ethics Board at the University of Alberta was granted for this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The authors agree in sharing the data on request.