Article Text

Abstract
Background As a response to the COVID-19 pandemic, most countries have adopted measures of social distance, with the childhood population being one of the main focus of attention in these measures.
Methods A rapid scoping review was carried out by searching PubMed to know if children are more contagious than adults, and the proportion of asymptomatic cases in children. Google Scholar and MedRxiv/bioRxiv were also searched. The time period was restricted from 1 December 2019 until 28 May 2020. Only studies published in English, Italian, French or Spanish were included.
Results Fourteen out of 1099 identified articles were finally included. Studies included cases from China (n=9 to 2143), China and Taiwan (n=536), Korea (n=1), Vietnam (n=1), Australia (n=9), Geneva (n=40), the Netherlands (n=116), Ireland (n=3) and Spain (population-based study of IgG, n=8243). Although no complete data were available, between 15% and 55%–60% were asymptomatic, and 75%–100% of cases were from family transmission. Studies analysing school transmission showed children as not a driver of transmission. Prevalence of COVID-19 IgG antibody in children <15 years was lower than the general population in the Spanish study.
Conclusions Children are not transmitters to a greater extent than adults. There is a need to improve the validity of epidemiological surveillance to solve current uncertainties, and to take into account social determinants and child health inequalities during and after the current pandemic.
- epidemiology
- virology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
The COVID-19 pandemic has changed the lives of families and children almost everywhere in the world.
Children are susceptible to COVID-19 although clinically they are present with milder symptoms compared with the elderly, and the general population.
Given the lack of effective treatment, measures taken by governments in several countries in order implement social distances included school closure, and even in some cases children were confined to the home.
These measures, mainly following the precautionary principle, were based on the experiences of previous epidemics (ie, influenza) where children were the main transmitters.
What this study adds?
Children are not transmitters to a greater extent than adults.
Many of the reported cases in children were from family transmission, and the percentage of asymptomatic children was variable (15%–60%).
The urgent need to improve the validity of epidemiological surveillance to solve current uncertainties.
Measures taken should balance the potential benefits and avoid other potential adverse effects such as increasing social inequalities in children and families.
Introduction
The COVID-19 pandemic started in late 2019 in China has represented a substantial change in the health of the population worldwide, especially for families and children.1 2 This pandemic and the lack of effective treatment so far until now highlight the need to take measures to prevent the spread of the infection. Measures adopted at the beginning of the pandemic in almost all countries were based on the available evidence of previous epidemics like influenza, where children were major transmitters of the disease, even more than adults.3 Nevertheless, it should also be taken into account the data available from the current pandemic given there are several unknown questions. In the current situation, measures taken to prevent the spread of the pandemic are generally based on the precautionary principle, and these measures should balance the potential side effects with the infection itself.
In the case of children, data available seem to indicate that they are equally susceptible to presenting infectious symptoms, although less severe compared with the adult population and the elderly.4 At the moment, there are no certainties about the possible causes of this situation. There is also insufficient information on the child population as a source of transmission of the infection. Despite this, in the majority of countries, one of the first measures adopted has been the closure of schools and even in some countries, such as Spain, the house confinement of all minors was specifically decided for at least 45 days.5 These strict measures taken with children present some controversies given that up to date there are many uncertainties regarding these issues in the current COVID-19 pandemic.
Given this situation and the uncertainty on the transmission mechanisms, prediction of severity, the spread of infection in asymptomatic patients or immunity after infection, a systematic scoping review of the published data was carried out to try to move forward in answering the following questions: are children more contagious than adults? Are they proportionally more asymptomatic?
Methods
A rapid scoping literature review was carried out by search in PubMed using the following terms: “coronavirus or COVID-19 or SARS-CoV-2” and “neonates or pediatric or infant or children or adolescence” and “transmission” to find reports of paediatric COVID-19. Google Scholar, MedRxiv/bioRxiv and secondary hand search have also been done. The time period was restricted to the last 6 months, from 1 December 2019 and updated until 28 May 2020. Available full texts and the reference lists of the relevant studies were reviewed.
Inclusion/exclusion criteria
All studies published in English, Italian, French or Spanish related to the transmission of COVID-19 in children were included, as well as those comparing the percentage of asymptomatic patients according to age and also the source of contagion when this was possible.
Studies that did not present data on childhood population were excluded, as well as those that focused the data exclusively on the level of severity and/or hospitalisations and/or paediatric intensive care units (PICU), or the treatment. All kind of studies (case series, cohort studies, comments, editorials, etc) were included although the emphasis was stated on those descriptive studies of cases. It is not ruled out that there may be some duplication in the cases included. A description of the results obtained was carried out. It was not attempted to rate the quality of included studies in this review.
Results
Of the 1099 initial titles, 73 articles were selected for reading the full text. Of these, 14 articles were finally included (figure 1).
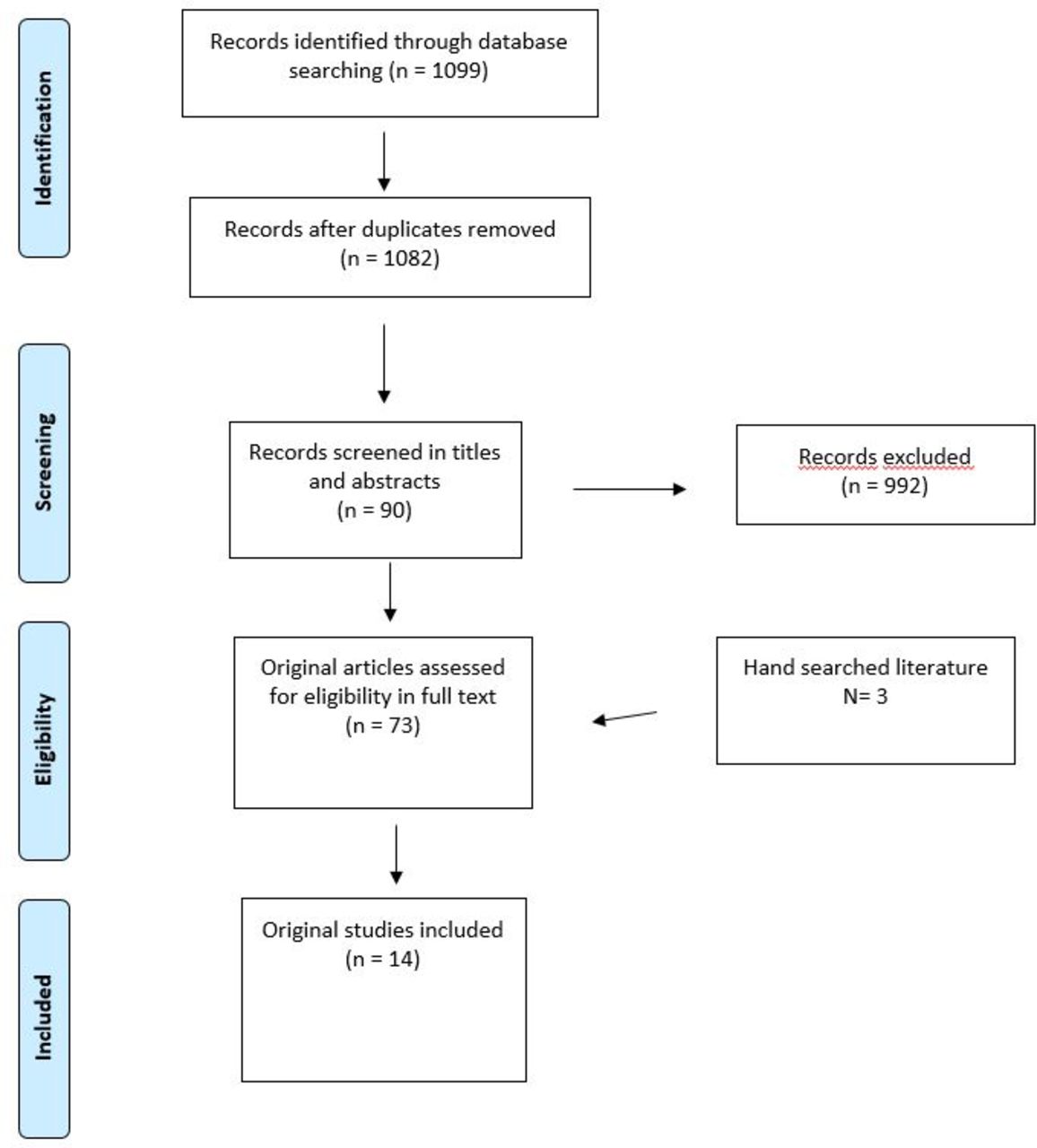
{kind=link}
Search flow.
Table 1 shows the results of included studies. Studies reported data from China, Taiwan, Korea, Vietnam, New South Wales (Australia), Geneva (Switzerland), the Netherlands, Ireland and Spain. Cao et al6 found that 2.1% of 44 672 confirmed cases were children or adolescents, mainly from intrafamiliar clusters. One of the larger series also based on the report of 2143 paediatric cases from China7 shows that 44% were asymptomatics and the main source of transmission seems to be the family (no data available). It should be taken into account that in the latter case series only 34% of cases of COVID-19 were confirmed and 66% were suspected cases.
Characteristics of included studies and main results
The first case reported from Korea8 (10 years old) and Vietnam9 (3 months old) was also associated with family transmission. A study from the hospital of Wuhan addressed to paediatric patients10 found that 171 out of 1391 screened cases were positive, 15% were asymptomatic cases and 90% of confirmed cases were from family transmission. A systematic review of 9 case series included 93 cases and reported that 26% were asymptomatics and 75% were from family transmission.11 Another series of 9 cases from 14 families,12 36 cases (out of 616 population)13 and 14 children (and 53 adults)14 found that 6, 18 and 8 children were asymptomatics, respectively.
All cases in children were from family transmission. In New South Wales schools, 9 cases of students of primary schools and high schools were reported, and 1 case was detected after 863 contacts analysed.15 A series of 40 cases out of 4710 at the general population were reported in children younger than 16 years from Geneva, and 8 cases were reported as case index.16
A study of households in the Netherlands reported data from 116 children 1–16 years and preliminary results showed that there are no indications that children younger than 12 years were the first in the family infected.17 In Ireland, no secondary school cases were detected after analysing 125–475 contacts of 3 detected cases in students 10–15 years old before school closures on 12 March 2020; 1 case was asymptomatic.18 Preliminary results of study of COVID-19 IgG prevalence carried out in Spain at the general population level indicate that minors have a lower prevalence of IgG antibodies than adults.19 In this study, the first results show that in children under 1 year, the prevalence of IgG was 1.1% (95% CI 0.3% to 3.8%), between 1 and 4 years=2.2% (1.4% to 3.6%), 5–9 years=3% (2.3% to 4.1%) and 10–14 years = 3.9% (3.1% to 4.9%), while in the general population the prevalence of IgG was 5% (4.7% to 5.4%).
Discussion
The results of the present review suggest that children are as likely to be asymptomatic cases as frequently as adults, and that a high percentage of reported cases came from family transmission. Although there are still many uncertainties, it does not appear that children are transmitters to a greater extent than adults. As previously mentioned, the drastic measures taken in the child population in several countries have probably been based on previous epidemics such as influenza,20 without enough evidence of the current situation. Moreover, there are some theoretical reasons why school closures may be less effective in COVID-19 than in influenza outbreaks. A systematic review found that modelling studies of COVID-19 predict that school closures alone would prevent only 2%–4% of deaths. This is much less than other social distancing interventions.21
No studies were found on the subject of the present review from France, Italy, or the USA, countries strongly affected by the pandemic. Studies from these countries to date have been addressed mainly to analyse severity of identified paediatric cases, the need of PICU or immune responses in children.22–24 Nevertheless, the results of this review are likely to be generalisable including cases from different countries. Two of the included studies analysing school contacts found a extremely low level of transmission at school.15 18 Moreover, other very recent published reviews show also the low role of children as a factor of transmission in general.25 26
Other secondary questions that come out from this review are the differences in the incubation period and the evidence that children (and probably also adults) can excrete the virus in faeces.6 According to some authors, asymptomatic individuals can actively shed the virus. Further, the incubation period in children following exposure to the virus can range upward of 24 days.27 Children more often have gastrointestinal symptoms compared with adults. The majority of children infected by novel COVID-19s have a documented household contact, often showing symptoms before them.4
If children are important in viral transmission and amplification, social and public health policies (eg, avoiding interaction with elderly people) could be established to slow transmission and protect vulnerable populations. Nevertheless, the application of the precautionary principle should be evidence based as much as possible and try to avoid creating adverse effects with potential medium and long-term negative impact on the childhood population. A study analysing viral load by age in a sample of 3712 patients from Berlin found no differences by age on viral loads, even in the very young patients do not differ significantly from those of adults.28
Several limitations of the present rapid scoping review should be mentioned. The inclusion of none reviewed preprint papers, the inclusion criteria based only on one evaluation, the lack of critical analysis of the risk of bias and the inclusion of non-primary study designs may weaken the attempts at understanding the data. However, the urgent need to understand the process of transmission and the results obtained provide a reasonable evidence on the process analysed. Furthermore, the results of other reviews on the process of infection in children with similar results to the present study support the strength of the results obtained. Another limitation is the current lack of reliable, valid and comparable data on epidemiological surveillance,29 on the diagnostic tests, and the scarce knowledge on the mechanism of transmission and prognostic.30 31 High-quality epidemiological studies are necessary to solve these questions with certain plausibility. On the other hand, up to date there are scarce data on the socioeconomic factors and its influence on the current pandemic. Social determinants of child health should be addressed to enhance the positive effects and avoid the adverse effects of this pandemic on children’s rights and social inequalities in children’s health.32
References
Footnotes
Twitter @LuisRajmil
Contributors I am the the only author that carried out this rapid scoping review, and have written the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data may be obtained from a third party and are not publicly available. Data will be available on reasonable request.