Article Text

Abstract
Objective To identify the birth prevalence of encephalocele in Africa, 2020.
Methods We carried out a systematic search of the following databases (PubMed/Medline, PubMed Central, Joanna Briggs Institute (JBI) Library, Cochrane Library, Web of Science, Google Scholar, Science Direct, African Journals Online and Embase), using search terms (prevalence, encephalocele, “neural tube defects”, “cranium bifidum”, “congenital malformations”, “congenital defects”, “structural birth defects”, “structural abnormalities”, newborns/neonates/ “live births”/ “stillbirths” and their MeSH Terms) up to 16 July 2021. The JBI quality appraisal checklist was used to assess the quality of studies when they were abstracted using a standardised data extraction template. The I2 statistic and Cochrane Q test were used to examine heterogeneity across studies statistically. The prevalence of encephalocele was estimated using a random-effect meta-analysis model. Subgroup, sensitivity, meta-regression and time trend analysis were carried out. The publication bias was checked using Egger and Begg’s tests.
Results Twenty-seven relevant studies were identified and provided a total of 5 107 109 births. In this systematic review and meta-analysis, the pooled birth prevalence of encephalocele in Africa was 0.02% (or 2 per 10 000 births) (95% CI 0.02% to 0.03%). The overall prevalence of birth encephalocele using the median from studies was 0.02% (IQR=0.01%–0.04%). Higher prevalence of encephalocele was detected in Nigeria 0.06% (95% CI 0.04% to 0.08%), Sudan 0.04% (95% CI 0.03% to 0.05%), Egypt 0.04% (95% CI 0.04% to 0.05%), DR of Congo 0.02% (95% CI 0.02% to 0.03%), Ethiopia 0.02% (95% CI −0.004% to 0.05%) and Tanzania 0.02% (95% CI 0.002% to 0.04%). The prevalence of encephalocele per live birth was 0.03% and both live birth and stillbirth was 0.03%.
Conclusions This review indicates a high prevalence of encephalocele, but studies were limited suggesting the need for additional research.
PROSPERO registration number CRD42021242161.
- epidemiology
- neonatology
- neurosurgery
- cell biology
- data collection
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. All relevant data are available within the manuscript. The data sets used and/or analysed during the current review are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Encephalocele is a birth abnormality associated with skull deformities defined by a partial absence of bone fusion that a portion of the brain protrudes.
It is one of the leading causes of death and disability in newborns.
What this study adds?
Although there are fragmented studies estimating the prevalence of encephalocele, there was no systematic review and meta-analysis on isolated encephalocele presenting this evidence.
This review highlights the birth prevalence of encephalocele in African countries, providing crucial evidence for policymakers, clinicians and the concerned bodies.
This systematic review and meta-analysis will contribute to assist the prevention and control programmes.
Introduction
Encephalocele is a birth abnormality associated with skull deformities defined by a partial absence of bone fusion, allowing a portion of the brain to protrude through a gap.1–3 It is a form of neural tube birth abnormality that affects the brain.2–6 The neural tube is a tiny canal that folds and closes to form the fetus’s brain and spinal cord during the third and fourth weeks of gestation.1 4 6
An opening will appear anywhere along the centre of the skull from the nose to the back of the neck following the defect, but most commonly at the back of the head, the top of the head or between the forehead and the nose.1 3 Encephalocele is a sac-like protrusion of the brain and meninges through a hole in the skull (usually affecting the occipital area, the back of the skull).2 6 The protruding region of the brain is frequently covered by skin or a thin membrane, giving the abnormality the appearance of a tiny sac.5 Its herniation process manifests as a pedunculated (with a stalk-like base) or sessile (with no stalk) cystic lesion.2 Only the meninges protrude through the bone opening in the sac, causing cranial meningocele; however, the herniated sac contains brain tissue and meninges, causing encephalocele or meningoencephalocele. Hydroencephalocele is a deformity that occurs when a herniated sac contains a ventricle. Encephalomyelocele is a type of encephalocele that contains tissue from the brain and spinal cord.1–9 Anatomically, encephalocele can be classified into sincipital (nasoorbital, frontoethmoidal, nasofrontal, interfrontal, nasoethmoidal, craniofacial cleft), basal (sphenoorbital, sphenomaxillary, intranasal, spenopharyngeal), convexity (sagittal, occipital, occipitocervical, parietal) and atretic.8 10 11 Evidence suggests that an encephalocele is a form of postneurulation defect distinct from closure-related neural tube defects.8 12
The incidence of encephalocele varies by race and geographical region, ranging from 0.8 to 4 per 10 000 births.7 8 11 According to the Centers for Disease Control and Prevention, encephalocele affects 1 out of every 10 000 babies born in the USA each year.1
The majority of encephaloceles are massive, serious birth abnormalities that are detected before delivery. Some encephaloceles, however, are small and go undetected in extremely uncommon circumstances. Although the specific aetiology of encephalocele is uncertain, scientists believe it is caused by a combination of causes.1–3
The symptoms of an encephalocele vary from person to person, based on a variety of characteristics such as the size, location, and amount and kind of brain tissue protruding from the skull. The placement of the encephalocele is crucial because anterior (which usually does not contain brain tissue and has a better prognosis) and posterior (often associated with neurological problems) encephaloceles have different clinical consequences/implications for therapy and prognosis. Surgical management is usually required to return the protruding section of the brain and meninges to the skull and shut the incision/opening. However, encephalocele-related neurological issues will persist, and long-term care may be required depending on the child’s condition.1 2
Encephalocele is the leading cause of death and disability in newborns,6 10 13 14 despite the fact that it can be reduced by various preventive and control strategies. Preventive strategies such as folic acid supplementation or fortification of staple foods can help to reduce it.3–6 13 14 In order to make decisions and plan preventative services, it is essential to provide information to responsible bodies concerning the burden of encephalocele in Africa. The government, policy-makers, health professionals, researchers, medical students, communities and non-governmental organisations will benefit from this review, which will help to reduce the burden of the encephalocele and allow for more study. Moreover, little is known about the magnitude of encephalocele in Africa as a whole. Thus, the present systematic review and meta-analysis aimed to identify the pooled birth prevalence of encephalocele in Africa, 2020
Methods
Reporting of the findings and review registration
Preferred Reporting Items for Systematic Reviews and Meta-Analyses statements were used to report the current systematic review and meta-analysis15 (online supplemental file 1). The review protocol has been registered in PROSPERO with the registration ID of CRD42021242161.
Supplemental material
Search strategies
PubMed/Medline, PubMed Central, Cochrane Library, Joanna Briggs Institute (JBI) Library, Science Direct, Web of Science, African Journals Online, WHO, UCSF and Embase databases were systematically searched for relevant studies (reference lists of identified articles were also navigated) up to 16 July 2021. The primary search was conducted in an advanced PubMed database (using search terms prevalence, encephalocele, “neural tube defects”, “cranium bifidum”, “congenital malformations”, “congenital defects”, “structural birth defects”, “structural abnormalities”, newborns/neonates/“live births”/“stillbirths” and their MeSH Terms). The core search terms and phrases were considered interchangeably in different databases. Moreover, grey literature was retrieved using Google and Google Scholar searches. The full search strategy is being shown online (online supplemental file 2).
Supplemental material
Eligibility criteria
Inclusion criteria
Published and unpublished full-text studies in any period and study designs (a cross-sectional, prospective cohort that included original data) that report the birth prevalence of encephalocele in Africa were included in this review.
Exclusion criteria
Case reports, conferences, editorials, anonymous reports and research with limited access (after two emails to the corresponding author) were excluded from the review. Moreover, a study was excluded if the total number of cases and births included in the study were not indicated explicitly.
Review outcomes
The outcome of the current review was the pooled birth prevalence of encephalocele in Africa. Birth prevalence of encephalocele is defined as the number of encephalocele cases of live births and/or stillbirths at birth (numerator) from the total number of births (live births and/or stillbirths) during the study period (denominator).
Quality assessment
The JBI quality appraisal checklist was used to evaluate the quality of each study.16 The JBI critical appraisal checklist (which has nine items) was adapted for the studies reporting the prevalence data (online supplemental file 3). Using the framework, two reviewers (MO and AD) independently evaluated the quality of each study. During the evaluation of quality, disagreements between reviewers were resolved by using the average score of the two reviewers. In the end, if the study received five or more points on all quality assessment items, it was deemed low risk.17
Supplemental material
Study selection and data abstraction
After retrieving all of the studies from the databases, they were loaded into the reference manager, an Endnote V.7 software program, to eliminate duplicates. The reviewers then screened the research for inclusion based on the title and abstract. All necessary data were extracted independently by two reviewers (MO and AD) using a defined data extraction template after thoroughly reading full-text studies and including the eligible studies. The main author, sample size, study nation, study duration, study design, study location, publication year, prevalence period, folic acid fortification policy, birth status, birth outcome and birth prevalence of encephalocele were all included in this template.
Meta-analysis
For further analysis, the data were extracted in Microsoft Excel and exported to STATA V.14 Statistical Software. For each study, the prevalence was estimated per hundred births to preserve uniformity.
The Cochrane Q test and the I2 statistic were used to examine statistically the heterogeneity between studies and a forest plot was used to visualise heterogeneity.18 This revealed considerable heterogeneity among studies (p<0.001). Therefore, to determine the pooled prevalence of encephalocele, a random-effect meta-analysis approach was applied.19 20 Subgroup analysis was performed based on selected variables (the study country, study design, birth outcome, folic acid fortification status, epidemiological design and status of births). A sensitivity analysis was done to see the influence of a single study on the overall estimate of meta-analysis. Meta-regression analysis was accounted for to identify the source of heterogeneity. A time-trend analysis was conducted as well.
Assessment of publication bias
Graphically, Egger’s plot was used to visualise the publication bias. Objectively, Egger’s regression test and Begg’s test statistics were used to detecting publication bias.21 22 As a result, publication bias was defined as a p≤of 0.05.
Patient and public involvement
‘No patient involved.’
Results
Study selection
A total of 5422 articles were initially retrieved on the prevalence of encephalocele through PubMed, Google Scholar and others from Cochrane, JBI Library, WHO, Medline, UCSF, African Journal Online, Science Direct and Embase. Of these, 1536 were excluded due to duplicated articles. From the remaining 3886 studies, 3660 studies were excluded after reviewing the titles and abstracts because they were found non-relevant for this review. Full texts of the remaining 226 studies were screened. This systematic review and meta-analysis comprised 27 studies that met the inclusion criteria23–49 (figure 1).

Study selection flow diagram; a figure adapted from the PRISMA group statement for this review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of the original studies
The included studies were either cross-sectional (n=4), retrospective (n=14) or prospective studies (n=9).23–49 Of all studies, eight were conducted in Nigeria,23–30 three in South Africa,31–33 two in Ethiopia,40 41 two in Tanzania,34 35 two in Kenya36 37 and two in Sudan.38 39 Studies conducted in Morocco, Tunisia, Algeria, the Democratic Republic (DR) of Congo, Egypt, Cameron, Ghana and Libya were also identified.42–49 All studies included in this review were facility-based studies, published in the year between 1992 and 2020.23–49 South Africa (started fortification in 2003), Nigeria (in 2002), Tanzania (in 2011) and Kenya (in 2012) have mandatory folic acid fortification with Wheat Flour and Maize Flour. Morocco (in 2006), Cameron (in 2011) and Ghana (in 2006) have mandatory folic acid fortification with Wheat Flour. Ethiopia and Sudan have a voluntary folic acid fortification policy with Wheat Flour at this time. Based on birth status, four studies mentioned the inclusion of twin birth and multiple births in addition to singleton births29 36 40 43 while all other studies not mentioned their birth status. Generally, 27 studies reported a total of 5 107 109 births, ranged from 1456 to 3 803889 births27 46 (table 1).
The characteristics of studies included in the systematic review and meta-analysis
Quality of the studies
Using JBI quality appraisal criteria, all included studies were evaluated for their quality. Each study was evaluated using the evaluation checklist for prevalence studies, which consists of nine questions/items with yes, no, unclear or not applicable responses. The quality assessment grading for all items was based on the JBI descriptions for each item. As a result, the studies’ quality scores ranged from four to nine. Therefore, except for one study that received a four, none of the studies had a significant risk of being of poor quality23–49 (online supplemental file 4).
Supplemental material
Meta-analysis
Prevalence of encephalocele
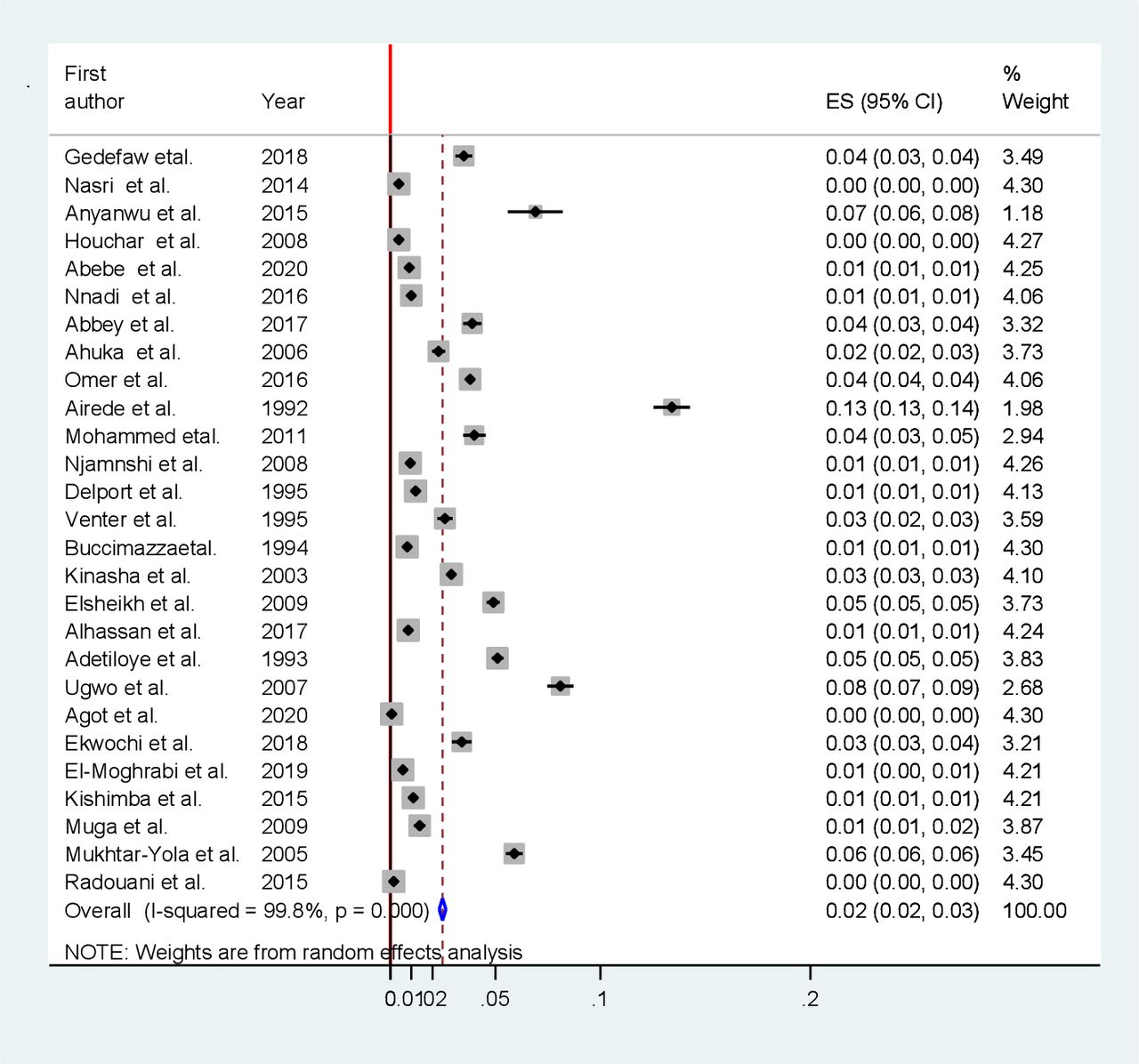
In the present meta-analysis, the pooled birth prevalence of encephalocele was 0.02% (or 2 per 10 000 births) (95% CI 0.02% to 0.03%). A Forest plot showed that there was statistically significant heterogeneity across the studies. Therefore, the random-effect meta-analysis model was applied to pool the overall prevalence of the studies (figure 2). Considering all included studies, the median value of birth encephalocele was 0.02% and the IQR was between 0.01% and 0.04%. The minimum and maximum values of birth encephalocele were 0.0007% and 0.134%, respectively (online supplemental file 5).
Supplemental material
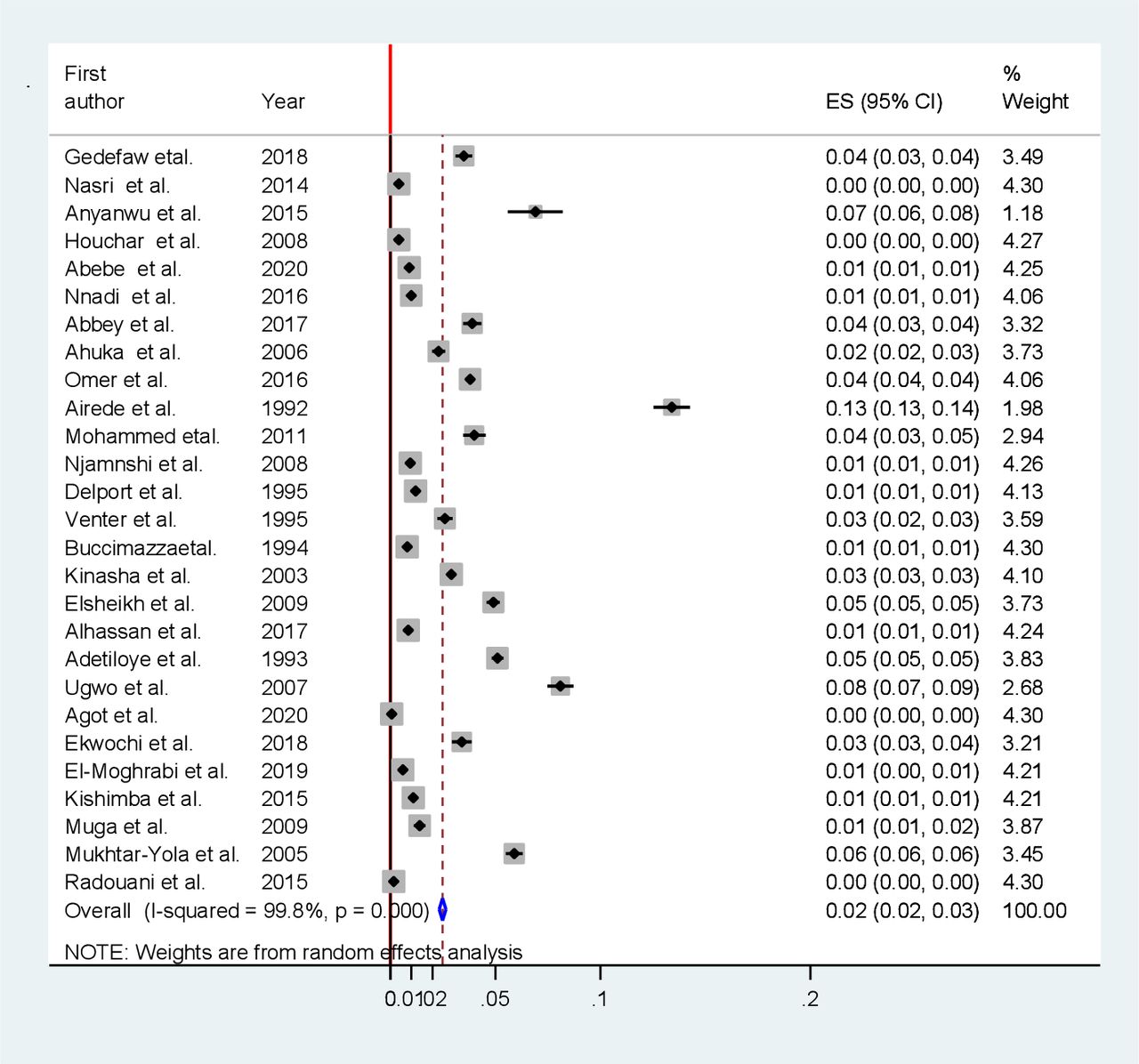
Forest plot showing the pooled prevalence of encephalocele in Africa. ES, Effect Size
Subgroup analysis
Subgroup analysis based on the study country, study design, birth outcome, folic acid fortification status, epidemiological design and status of births was carried out to see the variation of the prevalence across the studies.
Subgroup analysis based on the study country was performed to see the pooled prevalence of each country in Africa. High pooled prevalence of encephalocele was detected in Nigeria 0.06% (95% CI 0.04% to 0.08%), Sudan 0.04% (95% CI 0.03% to 0.05%), Egypt 0.04% (95% CI 0.04% to 0.05%), DR of Congo 0.02% (95% CI 0.02% to 0.03%), Ethiopia 0.02% (95% CI −0.004% to 0.05%) and Tanzania 0.02% (95% CI 0.002% to 0.04%) (table 2). In the present review, statistically significant heterogeneity between countries was detected (p=0.001, I2=97.1%–99.8%). Therefore, the Der Simonian and Laird’s (D+L) pooled prevalence method was considered because it is more conservative than the inverse variance method. The difference between countries was significant (p<0.001).
The pooled prevalence of encephalocele among African countries
Subgroup analysis based on study design, using the D+L method (p<0.001, I2=99.4%–99.9%), the prevalence of encephalocele for retrospective studies was 0.02% and for prospective studies was 0.04% (figure 3).
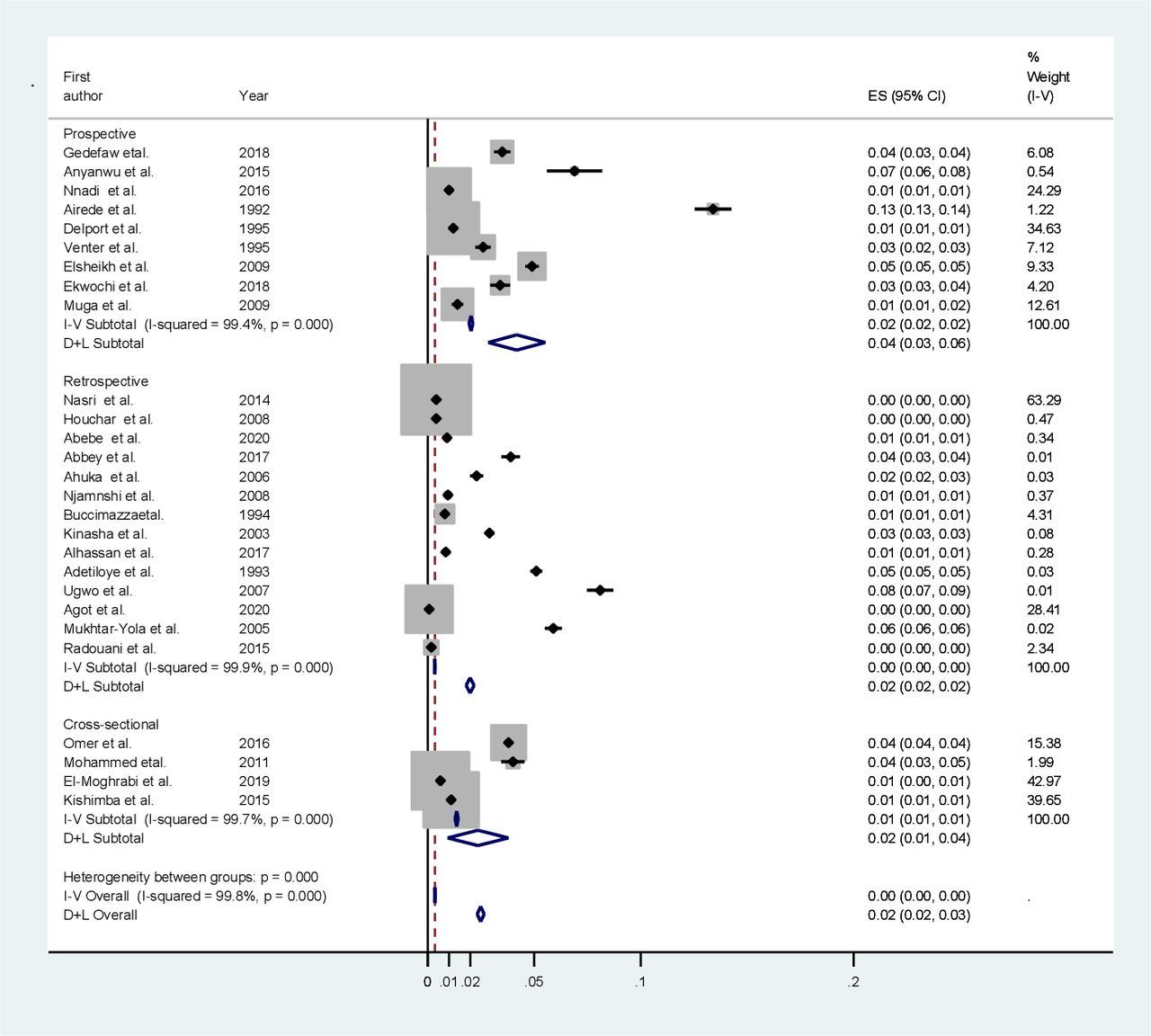
Subgroup analysis based on study design in Africa. ES, Effect Size
Subgroup analysis based on birth outcome was done to see the burden in live births only (LB) and both live births and stillbirths (LB +SB). The pooled prevalence of encephalocele per live birth was 0.03% (95% CI 0.02% to 0.04%) and both live birth and stillbirth was 0.03% (95% CI 0.02% to 0.03%) (figure 4).

Subgroup analysis based on birth outcome in Africa. ES, Effect Size; LB, Live Births; SB, Stillbirths
Subgroup analysis based on folic acid fortification policy was considered (p<0.001, I2=99.7%) and the prevalence of encephalocele for countries that had a mandatory and/or voluntary folic acid fortification was 0.03% (95% CI 0.02% to 0.03%), and for countries that had no either a mandatory or voluntary fortification was 0.03% (95% CI 0.02% to 0.03%).
The prevalence of encephalocele for incidence studies was 0.04% (95% CI 0.03% to 0.05%), for prevalence studies was 0.02% (95% CI 0.02% to 0.02%) and for prevalence case–control studies was 0.004% (95% CI 0.003% to 0.005%).
The prevalence of encephalocele for singleton births was 0.03% (95% CI 0.02% to 0.03%), for singleton and twin births was 0.02% (95% CI −0.01% to 0.05%) and for singleton, twin and multiple births was 0.03% (95% CI 0.002% to 0.05%).
Meta-regression analysis
In the present systematic review and meta-analysis, sample size (p=0.44), year of publication (p=0.34), duration of the study in months (p=0.20), study country (p=0.02), study design (p=0.56), birth outcome (p=0.55), epidemiological design (p=0.37), folic acid fortification (p=0.91), and the JBI quality score (p=0.06) were analysed for the source of heterogeneity. The only study country was significant for the source of heterogeneity.
Sensitivity analysis
In this review, no study was found that has a special influence over others on the overall estimation of meta-analysis (figure 5). Essentially, all studies have uniform confidence intervals. Sensitivity analysis does not help to explain heterogeneity because the heterogeneity between studies was not significantly reduced (p<0.001, I2=99.7%–99.8%), after doing the analysis with a few studies. We performed also leave-one-out analyses; the heterogeneity among studies was not significantly reduced.
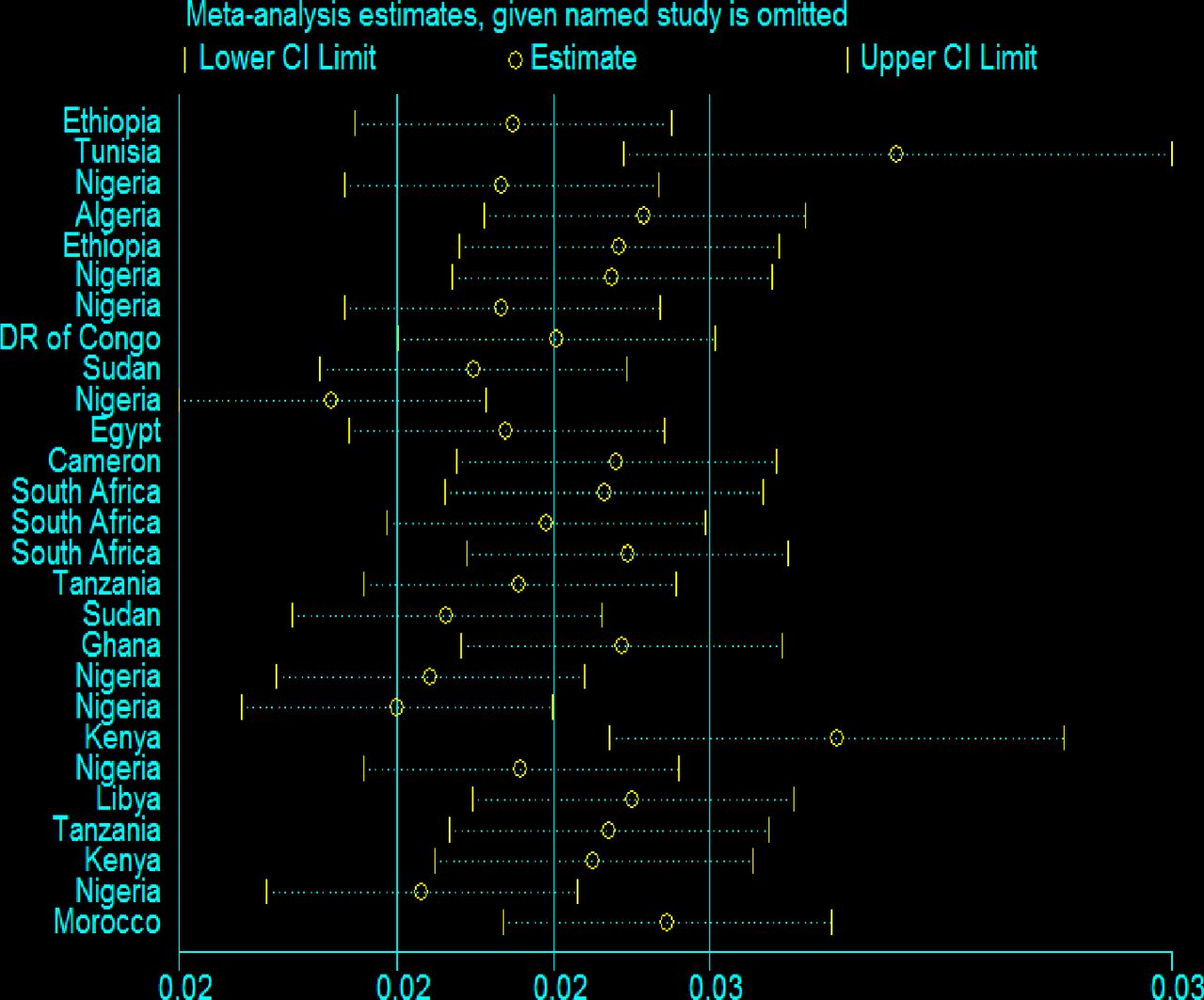
Sensitivity analysis to see the influence of each individual study in Africa.
We used sensitivity analysis to examine the impact of low-quality studies on total estimates by reducing the number of studies included in a meta-analysis. We found the meta-analysis estimates by including only high-quality studies with a score greater than or equal to five. As a result, we got a similar output with the previous finding and, the pooled estimate was 0.02% (95% CI 0.02% to 0.03%).
Time-trend analysis
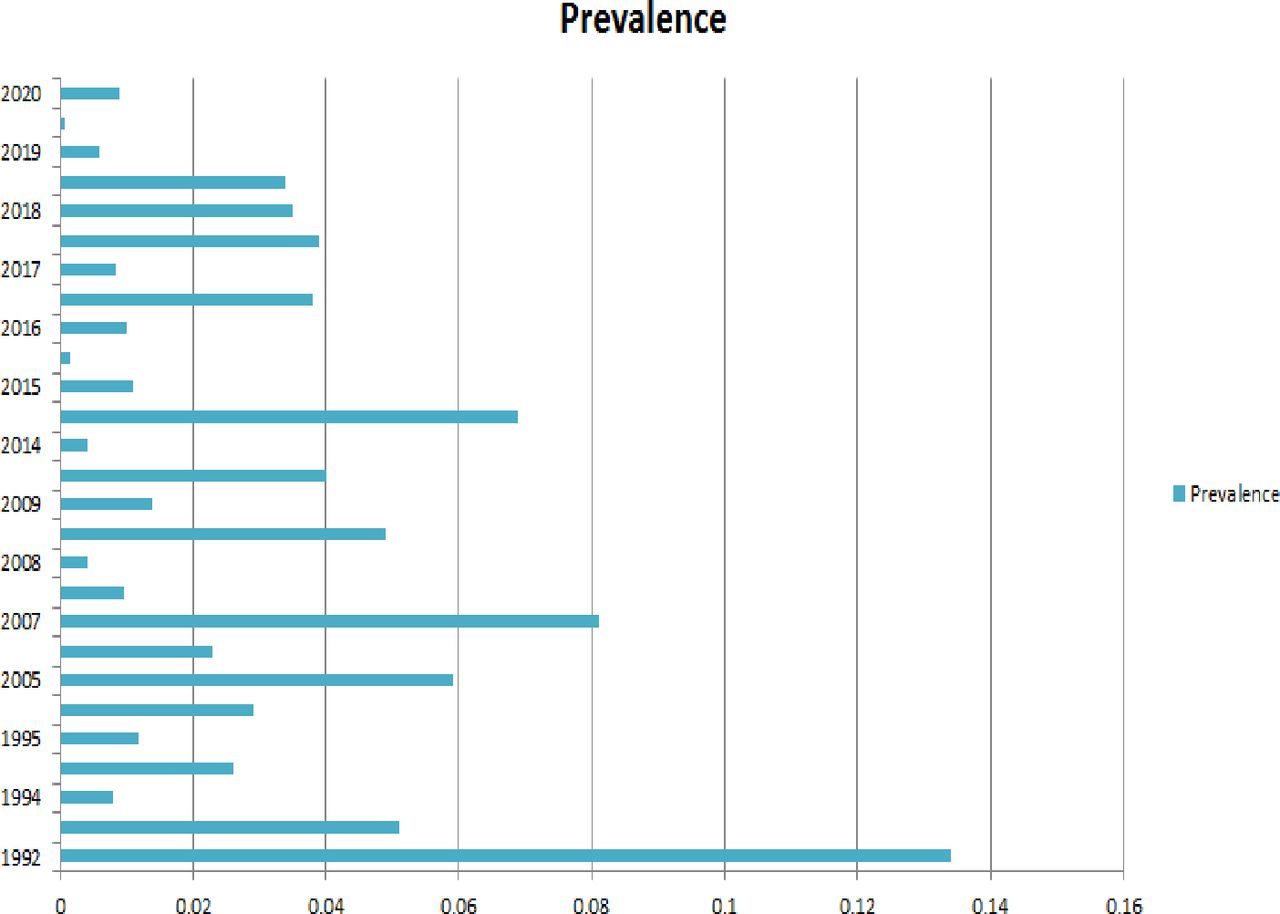
The time-trend analysis showed the relationship between the prevalence of encephalocele and publication year. In this trend in Africa, the highest peak of encephalocele in prevalence was observed in 1992, 2007, 2014–2015 and 2005 (figure 6).
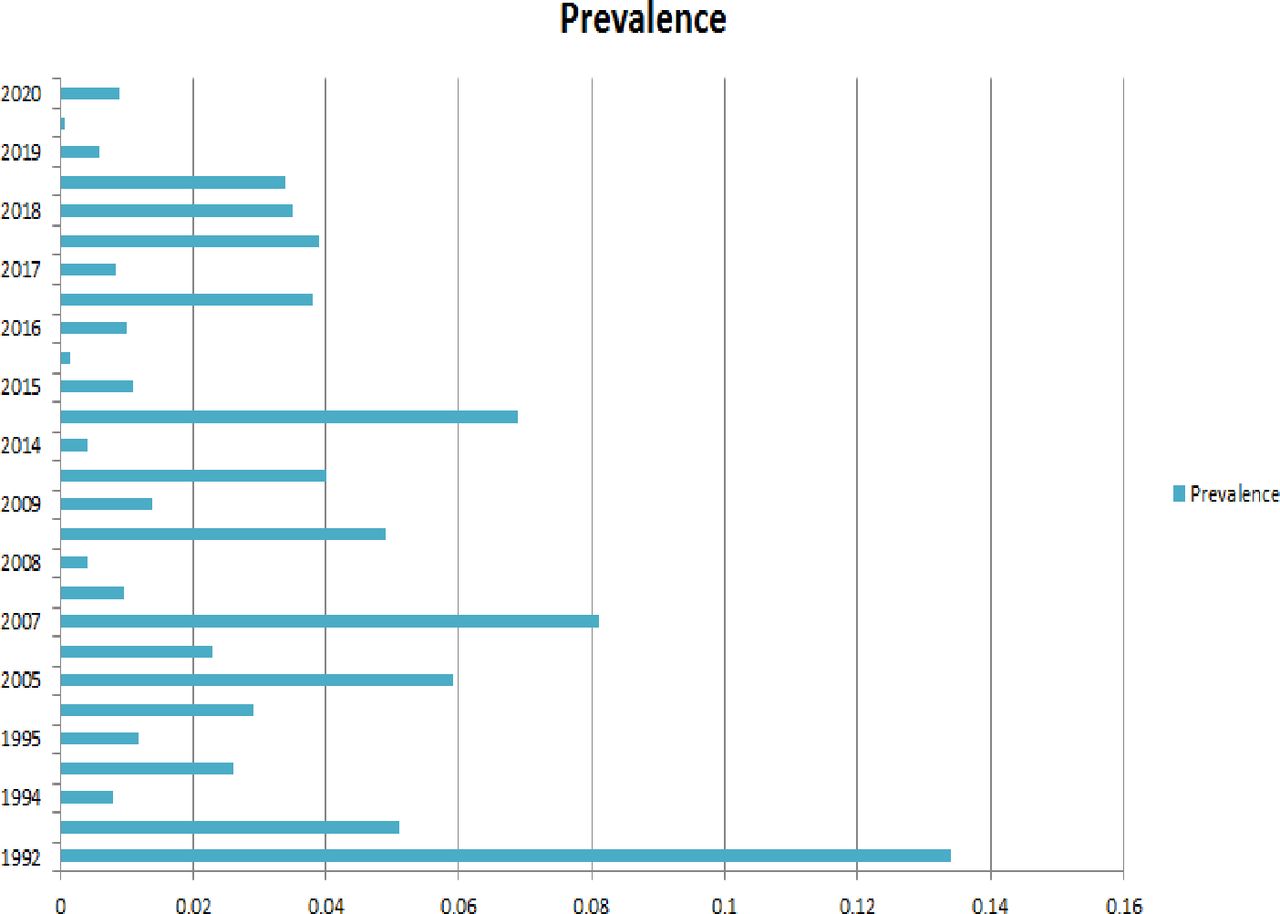
Time trend analysis of the prevalence of encephalocele in relation to publication year in Africa.
Publication bias
Publication bias was estimated using the Egger’s regression tests (B-coefficient of bias: 17; p=0.001). Egger’s plot supported its results (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Egger’s publication bias plot.
Discussion
Encephalocele is a central nervous system abnormality that occurs at birth. The hidden burden of encephalocele was high in Africa. Data is lacking on the true burden of this condition, leading to neglect in the treatment and prevention by health systems in Africa. The responsible authorities or bodies have neglected this defect too. The effects of the malformation are related to substantial mortality, disability and psychological costs (the psychosocial problem of having an infant with a ‘monstrous outlook’ or ‘two heads’). Although encephalocele is a rare congenital anomaly, it is correlated with severe morbidity and mortality if untreated.7 8 Folic acid supplementation and termination of pregnancies diagnosed with encephalocele prenatally have reduced the occurrence or incidence of this type of congenital abnormality, particularly in developed (high-income) countries.
The birth prevalence of encephalocele was 0.02% (or 2 per 10 000 births) in this meta-analysis. This finding is comparable to different findings reported elsewhere (ranged from 0.8 to 4.0 per 10 000 births).4–8 11 Besides, it is comparable to the review done in low-income and middle-income countries (2.1 per 10 000 births).50 The review result suggested that low-income and middle-income countries were mostly affected by this malformation every year.50 However, the review did not include studies from Africa except for two studies. Our finding is higher than that reported by certain high-income countries (1.0 per 10 000 births).1 Recent research shows that the prevalence of encephalocele varies across time, geography and population to population.8 Our analysis also revealed considerable differences between African countries and prevalence over time. Subgroup analyses were carried out based on the study nation, design, birth outcome, birth status and the availability of a folic acid fortification programme. As a result, a considerable disparity in the occurrence of encephalocele in different African countries was discovered in this study. Nigeria 0.06%, Sudan 0.04%, Egypt 0.04%, Congo (DR) 0.02%, Ethiopia 0.02% and Tanzania 0.02% had a high prevalence of encephalocele. This disparity could be explained by mothers’ levels of knowledge about folic acid supplementation, as well as the country’s health policy on folic acid fortification and other preventive measures. The notion of the presence of geographical variation between the countries was supported by the previous studies.6–8 The variation in different publication years of the different studies was noted using time trend analysis. The highest peak of encephalocele in prevalence was seen in 1992, 2007, 2014–2015 and 2005. The prevalence estimate for live births was similar to both live birth and stillbirth estimations. Surprisingly, all studies in this review were facility-based studies. Thus, there may have been an underestimating of encephalocele estimations because it did not include many stillbirths and home deliveries in the community context (included the participants delivered at the hospital setting).
The findings of the current systematic review and meta-analyses should be interpreted based on some limitations. The presence of significant variation across countries may affect/underestimate the pooled prevalence of the defect in Africa. Moreover, the prevalence estimate did not include terminated pregnancies of encephalocele; this may lower the pooled prevalence estimates. The estimated report may be influenced by the sample size’s adequacy or variability. Furthermore, publication bias was detected by Egger’s regression tests that may not decrease by trim and fill meta-analyses. Underestimation of the burden of encephalocele should be considered because many home births that are delivered in the community setting were not included. The review was represented by 27 studies due to limited available data about encephalocele.
Fragmented studies have been conducted to estimate the country-level prevalence of encephalocele. However, the findings were inconsistent and varied and there is no empirical evidence on the pooled prevalence estimates in Africa. Besides, studies on isolated encephaloceles are quite rare. The available evidence on encephalocele is in aggregate/combined form with either neural tube defects or birth defects of the central nervous system. Interestingly, the present systematic review and meta-analysis highlight the birth prevalence of encephalocele in African countries, providing crucial evidence for policy-makers, clinicians and the concerned bodies who neglected the burden of this defect. Recognising a high burden in Africa may initiate the policymakers to develop effective control and prevention strategies and may use their ultimate potential in reducing the burden of the encephalocele and making further research possible. Additionally, the high burden detected in our review may inform policymakers positively on policy decisions related to prevention efforts in Africa where policymakers may feel that this is not a big enough problem for prioritising prevention funds. The severity, the observed differences in prevalence estimate among countries, may contribute by informing clinical and policy guidelines in the prioritisation of interventions and maintaining robust surveillance systems that track or screen all pregnancy outcomes or all births in Africa. Besides, future research works might benefit from the information gained from the current review when designing and developing new studies. Furthermore, it helps additional clinical studies to focus on risk factors, prevention, intervention and psychosocial outcomes of the defect in isolated form. More research should be conducted in Africa to assess the effectiveness of folic acid in reducing the burden of the encephalocele and, notably, to determine how and why interventions either work or do not work in each country that followed either a mandatory or voluntary fortification policy. All these should be the ultimate contribution of this review to the field in assisting the prevention and control programmes.
Conclusion
This systematic review and meta-analysis showed that encephalocele is highly prevalent in Africa. The prevalence of encephalocele was high in Nigeria, Sudan, Egypt, DR of Congo, Ethiopia and Tanzania. A similar prevalence of encephalocele was observed in the studies that included only live births and in studies that included both live births and stillbirths. The reviewers recommend that special awareness be created for reproductive-age women with an emphasis on prevention in order to reduce the encephalocele burden. Due to the scarcity of data on encephalocele in Africa, more primary research is needed to increase the estimated burden of the encephalocele and promote favourable aid strategies for prevention.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. All relevant data are available within the manuscript. The data sets used and/or analysed during the current review are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MO and AD participated in the conceptualisation of the review protocol, formal analysis, methodology or study design, writing-original draft, interpretation, writing-review and editing, and approving the final draft. MO and AD: quality assessment, data extraction, and literature review. All authors read and approved the manuscript. MO act as the guarantor of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.