Article Text

Abstract
Background Asthma is the most common chronic condition of childhood. Leukotriene receptor antagonists (LTRAs) are included in international guidelines for children and young people (CYP), but there have been highly publicised concerns about potential adverse effects. The aim was to identify and understand the reported frequency of adverse drug reactions (ADRs) attributed to LTRAs in CYP with asthma.
Methods Embase, MEDLINE, PubMed and CINAHL were searched up to October 2020. Reference lists of eligible papers were manually screened. Eligible studies identified adverse events attributed to an LTRA in individuals aged between 0 and 18 years diagnosed with asthma. Four different tools were used to assess risk of bias or quality of data to accommodate the papers assessed.
Results The search identified 427 papers after deduplication; 15 were included (7 case reports, 7 case–controlled or cohort studies and 1 randomised control trial (RCT)). 7012 patients were recorded, of which 6853 received an LTRA. 13 papers examined the ADRs attributed to montelukast, one to pranlukast and one to unspecified LTRAs. After language standardisation, 48 ADRs were found, 20 of which were psychiatric disorders. Across all studies, the most commonly reported ADRs were ‘anxiety’, ‘sleep disorders’ and ‘mood disorders’. The frequency of ADRs could be calculated in seven of the eight studies. Applying standardised frequency terms to the prospective studies and RCT, there were 14 ‘common’ and ‘uncommon’ ADRs. ‘Common’ ADRs included ‘agitation/hyperactivity/irritability/nervousness’, ‘aggression’ and ‘headache’. The case reports showed a similar pattern, describing 46 different ADRs experienced by a total of eight patients.
Conclusions LTRAs have a wide range of suspected ADRs in CYP, predominantly gastrointestinal and neuropsychiatric disorders. Careful monitoring of CYP with asthma is required, both to assess and manage ADRs and to step treatment down when clinically stable.
PROSPERO registration number CRD42020209627.
- pharmacology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Available from corresponding author on request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Asthma is the most common chronic condition of childhood globally.
Leukotriene receptor antagonists are internationally recommended as a step-up therapy for patients with asthma whose asthma is not controlled by inhaled corticosteroids.
There have been highly publicised concerns and the addition of warnings to the packaging regarding leukotriene receptor antagonists adverse drug reactions.
What this study adds?
Leukotriene receptor antagonists have a wide range of suspected adverse drug reactions in children.
Neuropsychiatric and gastrointestinal adverse drug reactions are the most common.
Introduction
Asthma is a disease of airway inflammation and bronchoconstriction. It is the most common chronic disease of childhood globally, affecting more than 338 million children globally.1 2 The UK has the highest prevalence of childhood asthma symptoms in the world, with the National Health Service spending around 1 billion pounds each year on asthma care.3 4 Globally, the prevalence of asthma has been steadily increasing, and as a result, so has the prescribing of anti-asthma medication, with management guided by national and international guidelines.2 5–7
Leukotriene receptor antagonists (LTRAs) are a class of drugs used as a preventative treatment for asthma and are usually prescribed as an additional therapy for patients whose acute symptoms and attacks remain uncontrolled by inhaled corticosteroids.6–8 Montelukast, the originator drug in this class, has also been separately licenced for allergic rhinitis in some nations.9–11 Initially licenced in 1998, montelukast was the 16th most prescribed medication in 2020 globally.12 13
Medications come with potential harms such as adverse drug reactions (ADRs), defined as ‘an unwanted or harmful reaction which occurs after administration of drugs’ and ‘is suspected or known to be due to the drug(s)’.14 In March 2020 montelukast was marked with a boxed warning by the US Food and Drug Administration (FDA) and other agencies, warning of the potential severity of adverse events attributed to the labelled drug.15 There was particular concern regarding significant neuropsychiatric events associated with this drug. These included suicidal thoughts and actions, depression and sleeping problems.15–19
This systematic review aims to identify types of ADRs reported in the medical literature for children and young people (CYP) who use LTRAs and provide estimates of the frequency of these suspected ADRs.
Aims
The primary aim was to identify and understand the frequency of ADRs attributed to LTRA in CYP with asthma.
Methods
The protocol for this review was registered, a priori, in the International Prospective Register of Systematic Reviews. The review is reported as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and follows the guidance recommended in other methodological papers.20
Eligibility criteria
All primary research study designs including case reports, randomised control trials (RCT) and cohort studies were eligible. Narrative reviews were excluded. Eligible studies contained patients aged 0–18 years who were taking an LTRA as a preventative therapy for asthma, and the frequency of ADRs (number of patients who presented with a described ADR in a defined cohort) was described in the study report. For case reports, this criteria was understood as the presentation of a novel ADR following the administration of an LTRA. Adverse events as a consequence of LTRA non-prescribed dose (eg, overdose) were also excluded. Studies in which the evaluation of ADRs was not the primary objective, and which stated that the ADRs presented were not significantly different from the placebo were excluded as the attribution of the ADR to the LTRA could not be confirmed. Studies which contained both adult (18+ years) and paediatric data were eligible only if the relevant data (ADRs in CYP) were recorded separately from results in adults. Human studies in any language and with any publication date were included.
Search strategy and study selection
In September 2020, we searched MEDLINE, PubMed, Embase and CINAHL using a combination of Medical Subject Headings (MeSH) and free-text subject headings to include the research question (see online supplemental table S1, for complete search strategy). The primary author (EGD) screened the titles and abstracts of all identified studies before comparing the full texts of the remaining studies with the eligibility criteria. This process was repeated independently by the second author (CEMR-G) in October 2020. Subsequently the authors finalised the eligible studies; the senior author (DBH) resolved disagreements between the authors at the full-text stage. Using the same eligibility criteria, the reference lists of all eligible papers were additionally manually screened.
Supplemental material
Quality assessment
RCT21 (1/15), cohort or case–control studies22 (7/15) and case studies23 (7/15) were assessed for risk of bias or quality of data using appropriate assessment tools (online supplemental tables S2–S4).
Data extraction and synthesis
Data were extracted from the eligible studies into Microsoft Excel (Office 2016) (tables 1 and 2). When studies were reported in multiple publications, information (such as study design, placebo status, etc) was collected across the multiple publications to maximise the information available. In these cases, data duplication or accidental non-inclusion was avoided by comparing the study design, authors, study date and participant number across the publications to ensure the data originated from the same study. In cases where studies presented ADR data as percentages of a defined population, the numerical incidence of each adverse event was calculated.
Eligible studies
Primary outcome data
Following data extraction, the language used to describe the reported ADRs was standardised to facilitate data analysis and avoid ADR ambiguity. Medical Dictionary for Regulatory Activities (MedDRA) terminology, defined as ‘a rich and highly specific standardised medical terminology to facilitate sharing of regulatory information internationally for medical products used by humans’, was assigned to each ADR term reported to ensure a universal understanding of the given ADR term.24 Where the intention of the term used to describe an ADR was ambiguous, three authors (EGD, DBH and IS) independently assigned MedDRA terms based on the context of the reported ADR in question, before collectively confirming the terms (online supplemental table S5. Similar or matching controlled language ADR terms were subsequently grouped before being categorised by class organ system. Adverse events categorised under multiple MedDRA class organ systems were assigned to a single class organ system. Again, this process was conducted independently by the three authors (EGD, DBH and IS) before consensus was reached (online supplemental table S6).
Additionally, definitions of frequencies were described using Summary of Product Characteristics (SmPC) guidelines—an internationally used standardised regulatory framework.25
The frequencies of these standardised and grouped terms were collated (table 2). Frequency data from the prospective studies/RCT (table 3) and case reports (table 4) were additionally examined separately.
Estimated likelihood of ADR presentation reported in prospective studies and RCT
The ADRs recorded per case study
Statistical methods
Summary statistics were performed but meta-analysis was not conducted due to differences between studies.
Patient and public involvement
This systematic review included substantial input from VS to provide patient representative, as a representative of an existing patient advocacy group. This was to ensure the scope of the review, the data presented and the conclusions reached were informed by patient perspectives.
Results
After duplicates were removed, the search identified 427 papers. We excluded 383 papers based on the title and abstract, and a further 29 following full-text screening. Fifteen papers met the eligibility criteria (figure 1 and table 1). Eligible papers comprised seven case reports, seven case–controlled or cohort studies and one RCT. Four out of the eight studies were prospective. In total, 7012 patients were recorded, of which 6853 received an LTRA. Thirteen papers examined the ADRs attributed to montelukast, one to pranlukast and one to unspecified LTRAs. Further characteristics of the studies are presented in table 1.

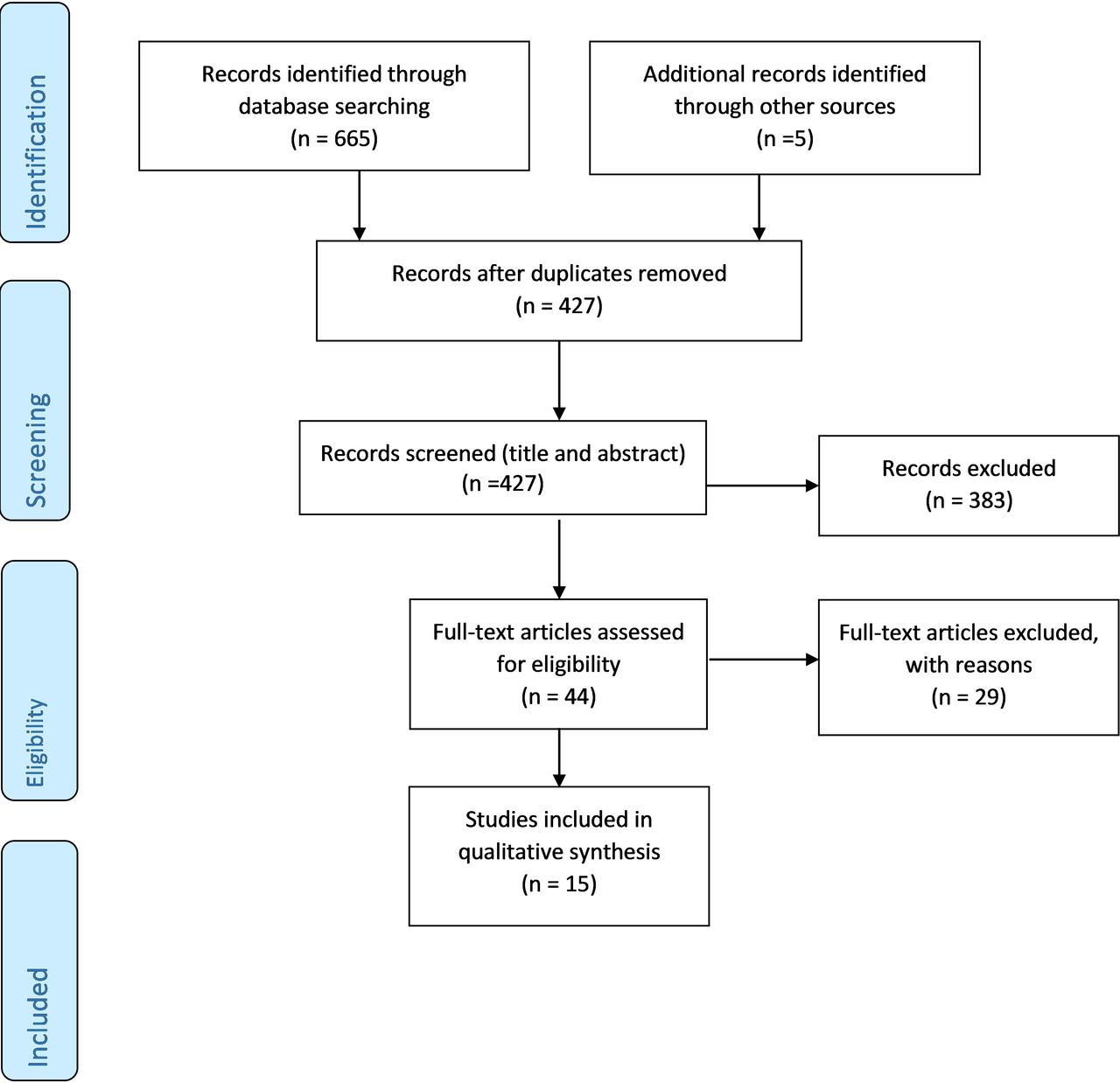{kind=link}
PRISMA flow diagram.
Risk of bias or quality of data assessment of included studies
Online supplemental tables S2–S4 show the results of the risk of bias and quality of data assessments for the 15 papers examined. The RCT was judged to have low risk. Four of the five case–controlled or cohort studies also had low risk (good), with one having some risk (fair) due to the selection process used. Both non-comparative studies showed good quality of data but demonstrated some uncertainly during post-intervention data recording. Lastly, four of the seven case studies had low risk of bias, with the remaining three having an unclear risk of bias in three of the eight criteria domains.
ADRs identified
A total of 73 different ADR terms were identified across the papers. Following language standardisation (online supplemental table S5), 48 distinct ADRs were identified and classified based on their class organ system (online supplemental table S6). The ADRs identified belonged to 13 different class organ systems.
Twenty of the 48 ADRs reported were classified as psychiatric disorders, the class organ system with the largest range of ADRs in this review. Additionally, ADRs in this class organ system appeared most frequently across the studies, with 10 of the 15 studies identifying at least one LTRA-induced psychiatric adverse event (table 2).
The most widely reported psychiatric disorders were ‘agitation/hyperactivity/nervousness/irritability’ (seven studies), ‘anxiety’ (six studies) and ‘sleep disorders’ (five studies). ADRs in the class organ systems of gastrointestinal disorders or nervous system disorders were the second most widely identified ADRs, appearing in 7 of the 15 studies each. The ADR of ‘abdominal pain’ was identified in all seven of the papers where a drug-induced gastrointestinal disorder was reported (table 2).
Frequency of ADRs identified
The frequency of the identified ADR was also recorded, classified as the number of patients who experienced the ADR within the population where that ADR was identified. The number of ADR events per patient was unknown in all but one study so was not included in this analysis (table 2).26
Without accounting for population size, the most frequently reported ADRs were ‘anxiety’, ‘sleep disorders’ and ‘mood disorders’. Twenty of the 48 ADRs were only identified in a single patient across all studies (table 2).
The frequency data from the prospective studies and RCT, and case reports (table 4 and online supplemental table S7) were additionally examined separately.
Attribution of frequency terms—prospective studies and RCT
Table 3 provides a breakdown of the frequencies of the ADRs by class organ system reported in the prospective studies and RCT.26–29 Following SmPC guidelines, a standardised frequency term was generated (very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10 000 to <1/1000); very rare (<1/10 000)).25 The total number of patients who were administered with an LTRA across the four prospective studies/RCT (1050 patients) was used as the denominator. Fourteen characterised ADRs were identified.
Common
Three ADRs were identified as being ‘common’ (≥1/100 to <1/10) as defined by SmPC documentation (table 3).25 This included two ADRs within the class organ system of psychiatric disorders and one nervous system disorders. The nervous system disorder of ‘headache’ was identified in two of the four studies. The other two ‘common’ ADRs were ‘agitation/hyperactivity/irritability/nervousness’ and ‘aggression’ and were only identified in one of the four studies each.
Uncommon
Eleven ADRs were identified as being ‘uncommon’ (≥1/1000 to <1/100) as defined by SmPC documentation (table 3).25 Each ADR was only identified in one of the four prospective studies/RCT.
None of the ADRs identified across the prospective studies or RCT had a presentation likelihood frequency of rare (≥1/10 000 to <1/1000) or very rare (<1/10 000).
Case report data
Online supplemental table S7 depicts a breakdown of the frequencies of the ADRs by class organ system reported in the case reports. As the patients in the case reports were identified due to presenting an LTRA-induced ADR, a likelihood calculation was inappropriate. Thirty-seven different ADRs were identified across the seven case reports. Fifteen different ADRs were included in the class organ system of psychiatric disorders, the largest number of ADRs out of the eight identified class organ systems. Psychiatric disorders were found most commonly across the seven case reports with five of the seven reports identify an ADR in this class organ system.
Forty-six different ADRs were experienced by a total of eight patients (table 4). All but one patient30 presented with ≤3 different ADRs, with one patient presenting 12 different ADRs across four class organ systems.31
Discussion
Without accounting for the population size of the studies or trials, the most frequently reported ADRs across all studies were ‘anxiety’, ‘sleep disorders’ and ‘mood disorders’. With 15%–30% of 2–5 years old and 11%–15% of 6–12 years old have behavioural sleep problems, these ADRs can be challenging to diagnose, especially when LTRA can induce an ADR at any point after drug administration.32 33 Clinical teams need to be aware of these ADRs as they are common in the child population and may alter the risk benefit profile of the drug.34
Montelukast is associated with a high frequency of neuropsychiatric ADR reports, including rare accounts of suicide,18 but there are other systems, notably the gastrointestinal tract, where ADRs are also regularly reported. This is well aligned with the UK national spontaneous reporting (Yellow Card) data from the Medicines and Healthcare products Regulatory Agency.35 Additionally, single large doses taken in error by CYP show predominantly gastrointestinal ADRs, with neuropsychiatric ADRs being less common.36
It is important not to view suspected ADRs in isolation, as LTRAs are an efficacious preventative treatment for asthma.6 7 37 38 Many randomised double-blind comparative studies have demonstrated montelukast’s anti-inflammatory mechanism of action; both its ability to cause significant reductions in peripheral blood eosinophils and fractional exhaled nitric oxide (demonstrative of reduced airway inflammation) in children have been widely documented.38–40
However, all new prescriptions and reviews of patients on existing medication should take account of the potential risks and benefits and evolving evidence in these areas. Recently, the FDA updated montelukast’s prescribing information document, acknowledging that the original clinical trials demonstrated that montelukast crosses the blood–brain barrier in substantial levels and not minimal levels as originally reported.32 41 Further evidence of montelukast’s direct action on the brain was demonstrated in young murine models, where montelukast caused a decrease in the proliferation of neurons in the hippocampal region.42 Importantly, the prescribing information document states that neuropsychiatric events have been also reported following montelukast discontinuation.32 It is therefore a useful time to collate and review the known and suspected ADRs in children who use this medication to provide clinicians with the most up-to-date information.
Limitations of this review are primarily related to the way ADR data were presented, with only one clinical trial reporting the number of times that each ADR occurred in an individual and none reporting the time period over which the ADRs occurred.26 Additionally, the proportion of patients who experienced multiple different ADRs is unknown, and it is not clear whether patients with multiple ADRs were within a single class organ system, or across a variety. This has prevented identification of any patterns of ADRs within or across systems and prevented the application of severity scores.
It is also possible that the review’s exclusion of studies where the ADRs presented were not significantly different from the placebo may have introduced bias through the potential exclusion of ADR data. However, false positives or ‘background noise’ are commonly reported in patients and healthy volunteers.43 44 Studies examining ADR presentation should acknowledge the presence of false positives prior to the commencement of an ADR investigation.
At a population level, removing unnecessary step-up therapies such as montelukast when asthma is deemed ‘stable’ is encouraged by international guidelines.6 7 However, the definition of ‘stable asthma’ is not clearly defined, and clinicians reviewing CYP with asthma who already using LTRAs will need to consider both the potential impact of stepping down therapy, as well the potential ADRs that may be occurring. We hope that this review will help structure the review of potential ADRs, helping to determine the appropriate treatment plan for an individual child.
Conclusion
LTRAs have a wide range of suspected ADRs in children, predominantly neuropsychiatric and gastrointestinal. To minimise the potential harms from ADRs, clinicians need to be aware of, and screen for, these ADRs. Careful monitoring of CYP with asthma is required, both to assess and manage ADRs and to step treatment down when clinically stable.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Available from corresponding author on request.
Ethics statements
Patient consent for publication
Acknowledgments
This is a summary of independent research carried out at the National Institute for Health Research (NIHR) Alder Hey Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the National Health Service, the NIHR or the Department of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @pharmaforkids
Contributors EGD conducted the systematic review. This included establishing the eligibility criteria, conducting the search, collecting the data and analysing the results. CEMR-G conducted the data search in parallel and compared eligible papers with EGD. VS advised and provided information on known leukotriene receptor antagonist (LTRA)-induced adverse drug reaction (ADR) cases and LTRA policy. IS and DBH equally oversaw the direction of the review including editing the writing of the paper, acted as consultants in characterising ADRs and ensured clinical relevance to the review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer This is a summary of independent research fcarried out at the National Institute for Health Research (NIHR), Alder Hey Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests VS has close relationships with individuals and families who identify as being adversely affected by montelukast side effects.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.