Article Text

Abstract
In 2020, 21% of people who sought asylum in the UK were children. This population has complex interconnecting health and social needs. Assessment requires a holistic approach, with consideration of physical and mental health in addition to social and developmental well-being, within the whole family group. A trauma-informed life-cycle and intergenerational care approach is important. This article, aimed at all health professionals who may work with asylum-seeking families, outlines the best practice principles for undertaking health assessments in migrant children and young people.
- Adolescent Health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
We are living in an age of increasing global humanitarian crises as a result of conflict, political and economic inequality, natural disasters and the effects of climate change, among other factors. An increasing number of young people and families are being forced to flee their homes in search of safety, food security, health, education and employment. At the end of 2020, 36 041 people claimed asylum in the UK.1 Of the 21% who were children, nearly one-third were unaccompanied minors.1 Reliable data regarding patterns of healthcare access and usage by accompanied and unaccompanied asylum-seeking children and young people (CYP) is limited, but it is likely that all paediatricians, emergency medicine clinicians, general practitioners (GPs), and most other healthcare professionals (HCPs) will encounter asylum-seeking CYP (table 1). Few HCPs in the UK have received specific training in the assessment of health needs of this group. These young people have complex physical and mental health needs and require a tailored approach with adherence to the principles of trauma-informed care. Younger children may have neurodevelopmental needs requiring follow-up or specialist care. There is a wide variation in the standard of care and services currently received by this patient group in the UK and Europe. This article aims to provide clinicians and allied health professionals with a framework for a ‘gold-standard‘ approach to comprehensive health assessments for asylum-seeking CYP. This will not only benefit patients themselves but also HCPs and clinical services by supporting provision of a high-quality, standardised and efficient service.
Definitions of displaced people
How to approach the assessment of asylum-seeking children
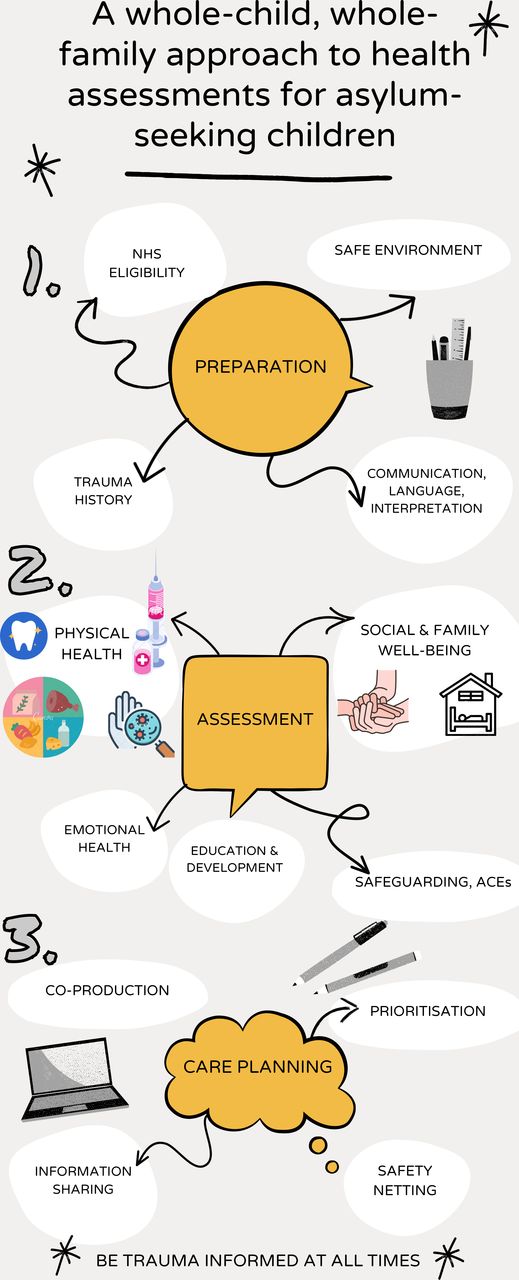
We propose that the optimal approach to carrying out health assessments in asylum-seeking CYP can be divided into three components of equal importance: the preparation phase, the health assessment itself and the formulation of the post-assessment healthcare plan (figure 1).

A whole-child, whole-family approach to health assessments for asylum-seeking children.
Preparation phase
This phase aims to assist professionals in preparing for the health assessment of the asylum-seeking child, while encouraging reflection about existing systems in their place of work. Professionals should think holistically and feel empowered to challenge and break down barriers that may hamper equitable healthcare access for migrant populations.
Preparation is also an essential component of trauma-informed practice2 (figure 2). Trauma-informed principles are essential pillars for professionals working with trauma survivors. For example, they provide guidance on how to make individuals feel safe during a consultation, how to ensure they feel empowered to make shared decisions about their care and how to avoid questions about potentially triggering events, particularly if this information is not needed to guide a practitioner’s specific area of clinical assessment and management. Before meeting with an asylum-seeking family, clinicians should consider ‘Has this person/family reported traumatic events? If so, how might these experiences influence their clinical presentation?’

Principles of trauma-informed care.
Clinicians may receive referrals from a range of professionals including; council workers of refugee resettlement programmes, welfare officers of private housing organisations, GPs, health visitors, school nurses, secondary care providers, tuberculosis screening services or voluntary organisations. Attendances may also be unscheduled, through emergency services or admissions. Most regions in the UK do not have formal referral pathways for refugees and asylum-seekers and National Health Service (NHS) digital platforms do not always facilitate the identification of, and information collection regarding, migrants and their settlement status. This problem is compounded by concerns about stigmatisation and the risk of such data being made available beyond the healthcare arena. This results in a lack of information around healthcare needs, access and outcomes of migrant CYP.3
Healthcare interventions are often opportunistic and rely on education, awareness, vigilance and motivation of the HCP, with a willingness to look beyond the presenting issue to identify other areas of need.
Planning can help to minimise communication barriers linked to language, trust and confidentiality (box 1). Collating documentation from previous health encounters is important, as care is often fragmented. Identification and preparation for an in-person or telephone translator in the correct dialect and language or a male/female practitioner according to patient preference is also crucial.
Overcoming communication barriers49
How to overcome communication barriers
Build trust by explaining the purpose of the appointment and giving reassurance about confidentiality.
Do not use family members, friends or untrained members of staff as translators in a medical consultation.
Use official interpreters (either face to face or remote organisations from high-quality and sustainable companies making sure they are using the correct language and dialect.
When using an interpreter, look/speak directly to the patient and use additional non-verbal communication cues when helpful.
Use trauma-informed care principles and offer to see adolescent patients alone but with an awareness aware of cultural needs (eg, a young female adolescent may not be comfortable being alone with a male doctor without a chaperone).
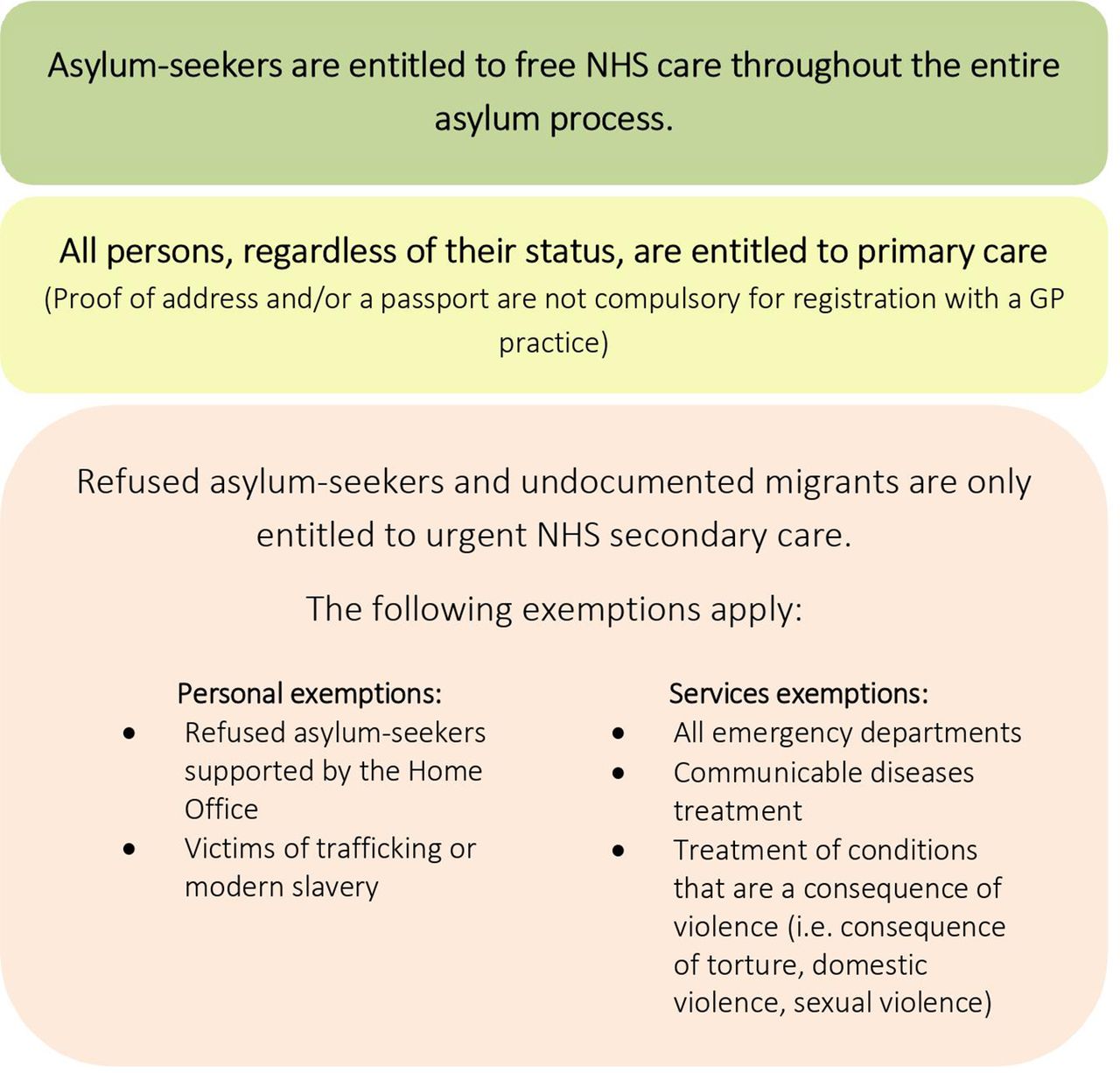
At the start of the consultation, it should be clarified that HCPs are not linked in any way to the Home Office and that medical records will not be shared with the Home Office or other authorities, unless under specific, legal, instructions (figure 3). It should, however, be explained that if it’s in the child’s best interest, information may be shared with other HCPs.
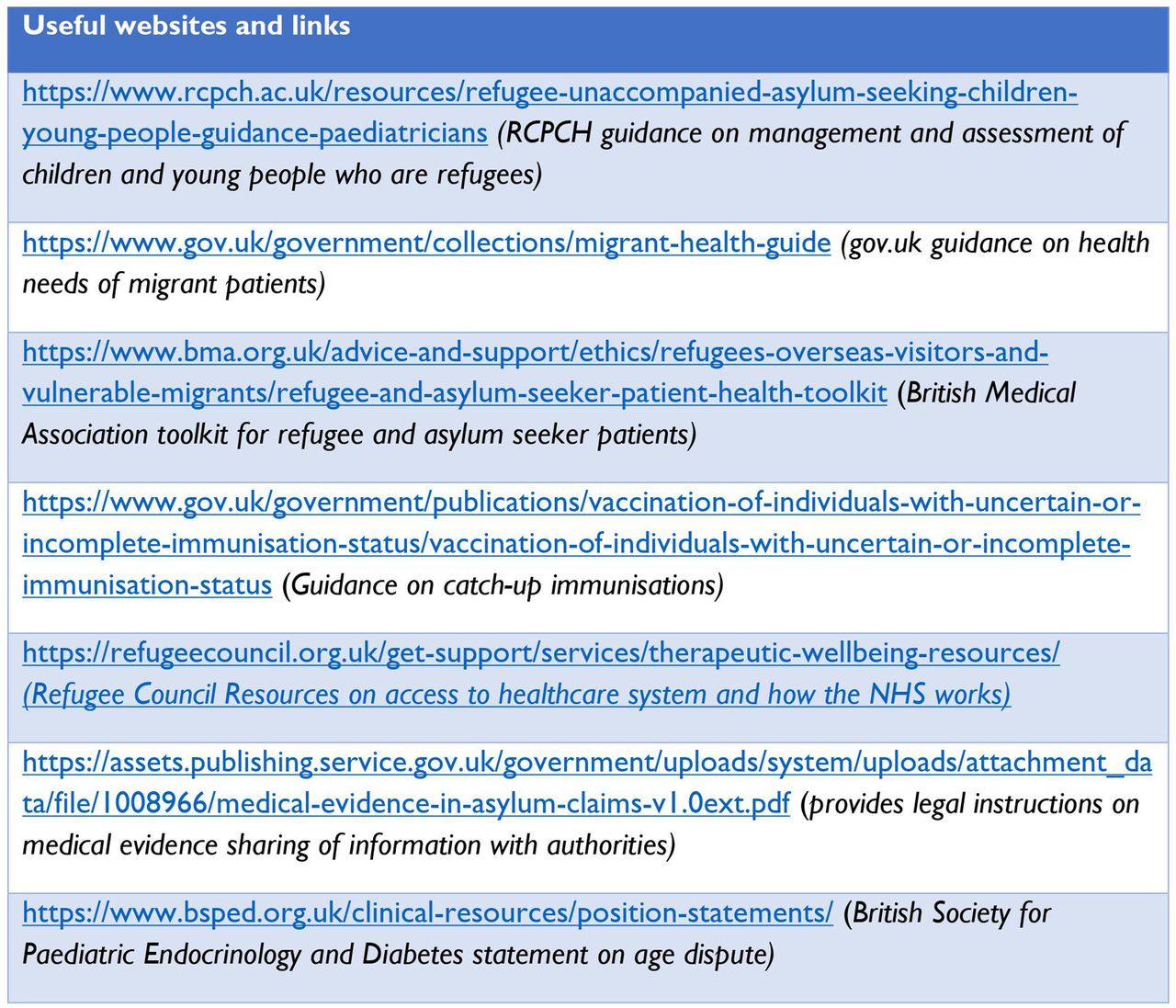
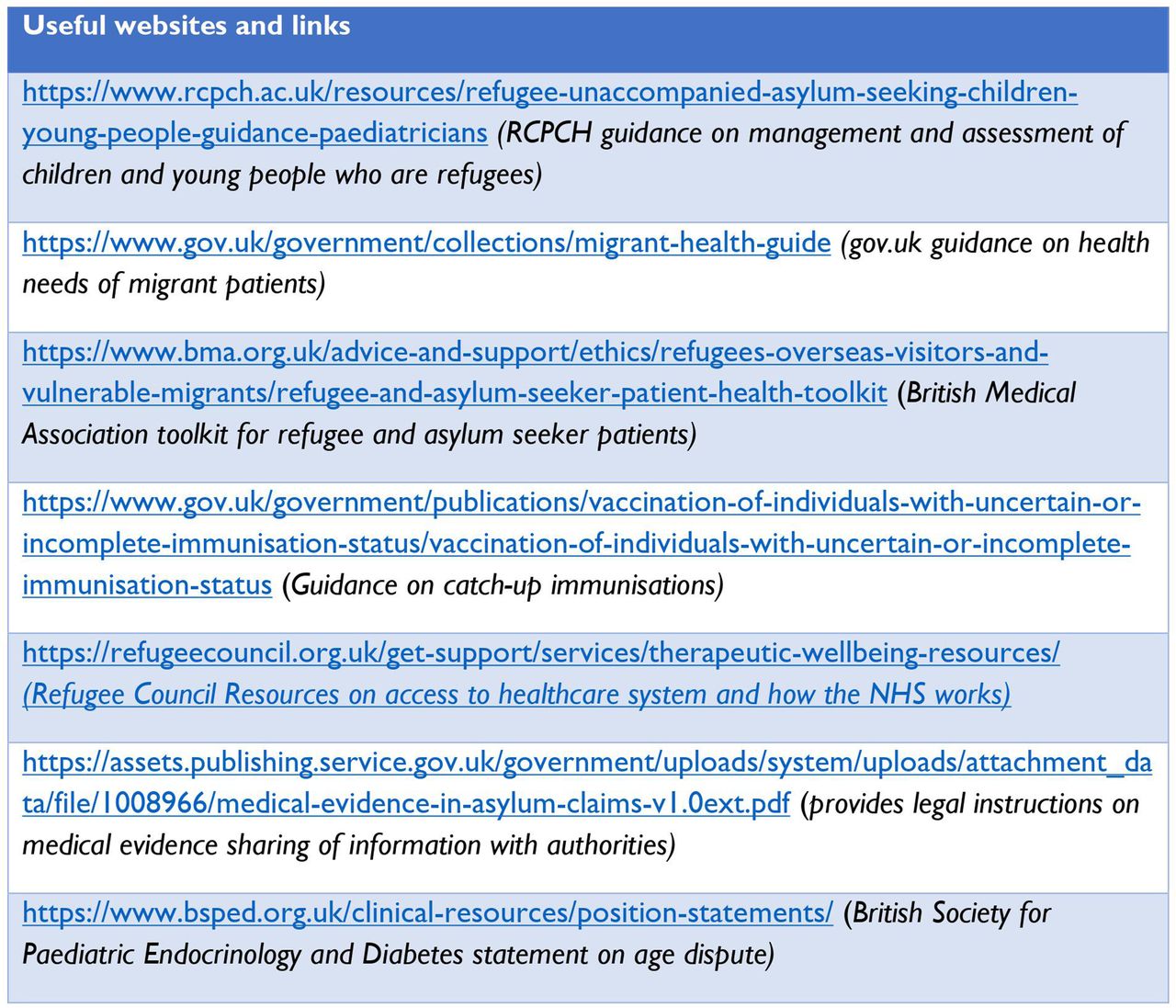
Useful links and websites. RCPCH, Royal College of Paediatrics and Child Health.
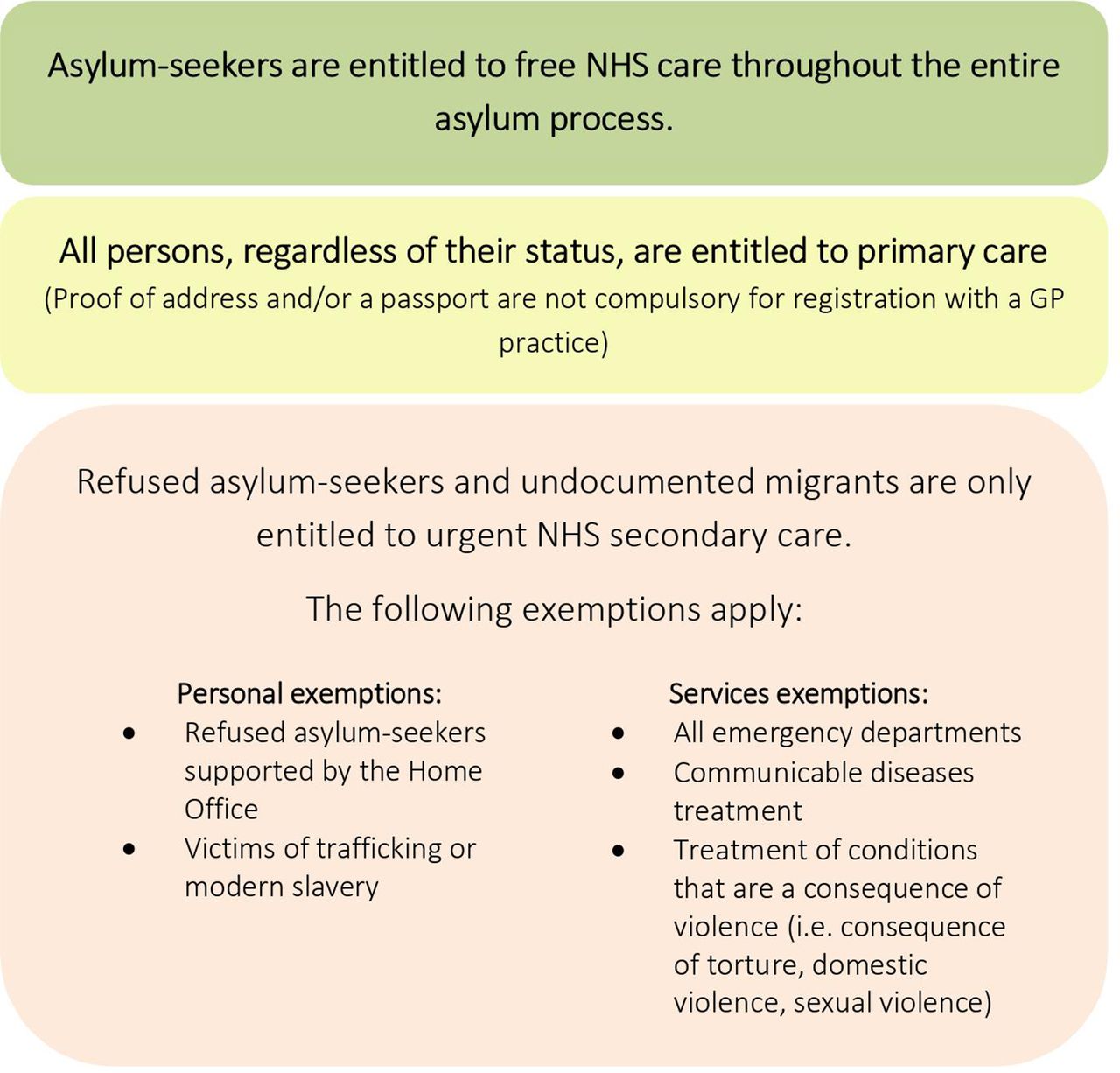
Clinicians should familiarise themselves with guidance around the right to access healthcare in the UK and be aware that asylum-seekers are exempt from NHS charging (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Right to access to healthcare for asylum-seekers in the UK. GP, general practitioner; NHS, National Health Service.
Health assessment
The health of asylum-seeking CYP is influenced by multiple, interconnecting factors (table 2).4 Migrant children have a higher prevalence of both physical and mental health problems compared with their peers.4–7 HCPs looking after these children should ideally have experience in addressing physical and mental determinants of health,8 and be aware that somatisation is a relatively common problem.9
Factors that may contribute to a poor health status of asylum-seeking children and young people on arrival
The well-being of a child is not only determined by their own health needs and experiences, but also influenced by that of parents and siblings. In the case of unaccompanied CYP, separation from the family, as well as other adverse childhood experiences,10 can contribute to psychological problems that may impact physical, mental and social development.11
Trauma in one generation can influence the development and well-being of the next generation,12–14 a phenomenon described as the intergenerational transmission of trauma. Parental mental health issues, such as post-traumatic stress disorder (PTSD) and depression, represent one mechanism through which trauma and ill health may affect the health of subsequent generations.14 15 Other mechanisms include maternal malnutrition leading to poor neonatal outcomes such as low birth weight and small-for-gestational-age15 and later infant or childhood malnutrition and stunting. This, in turn, may impact on risk of infections, poor cognitive development, concurrent stunting and obesity, non-communicable diseases,15 lower quality of life and lower income in adulthood.16
This complex and intergenerational matrix of needs underpins the requirement for holistic screening involving the whole family unit, where possible, to provide not only clinical expertise but also signposting and referral to other health services such as dentistry, optometry, social and psychological support, as well as educational opportunities and health promotional interventions such as primary immunisations, childhood multivitamins and dental fluoride varnish application. Some of the aspects to consider in paediatric migrant screening programmes are listed below and summarised in Table 3.
Aspects of the health assessment
Origin and journey
CYP who migrate with or without their families have often suffered traumatic, violent, exploitative or sexually abusive experiences prior to, and during, their journey, which will impact physical and psychosocial health (box 1). Obtaining a description of the migration journey is important but ideally should only be done once for the whole family using trauma-informed care principles.2 A balance must be sought between gaining adequate understanding of a child’s background in order to make safe health decisions and avoiding retraumatisation.
Current and past medical history
The paediatrician should ask about antenatal and birth history as well as any newborn screening undertaken in their country of origin. Family history may help in identifying genetic conditions and exposure to infections, as well as highlighting possible traumatic separation from other key family members. Most recent visits to dentists, audiologists and opticians can also be discussed, bearing in mind that many children may have had no prior access to these services.17 18
Physical health assessment
Physical health assessments should be comprehensive and follow available guidance from the Public Health England Migrant Health guide,19 as well as the most up-to-date evidence-based guidelines such as the latest Royal College of Paediatrics and Child Health (RCPCH) guidance for HCPs on accompanied and unaccompanied refugee and asylum-seeking children.5 20 Migrant populations commonly have many unmet health needs, undiagnosed or undermanaged chronic health conditions, such as haemoglobinopathies, poor dentition, common childhood conditions such as eczema and constipation as well as poor overall health as a result of limited access to screening and health prevention in their countries of origin or transit. Physical symptoms should be investigated but, if no organic cause is found, clinicians should be aware of potential somatisation or the effect of psychological distress on symptoms.21 Non-specific and medically unexplained symptoms such as body or limb pain, headache and dizziness, and abdominal pain are common and were found in around a quarter of unaccompanied asylum-seeking children (UASC) presenting to a London service.6
Documentation is crucial in this group who move around frequently and who are at risk of retraumatisation if histories have to be frequently repeated. Clear documentation of physical evidence of trauma or torture using a body map can be vital for home office assessment outcomes.
Infectious diseases screening
We recommend a comprehensive approach to screening for asymptomatic infections with blood and stool samples (table 3).19 An alternative approach to the latter, is universal antiparasitic treatment with albendazole for children from high incidence countries. Screening for sexually transmitted infections is also recommended in all postpubertal children, particularly given that there is a high rate of sexual violence suffered prior to and during migration journeys.6 Skin infestations such as scabies may be present and looked for, particularly in those that have spent significant time in refugee camps. Their journey to the UK is often long, transiting through many countries, leading to multiple opportunities for exposure to pathogens.
Summary of screening assessments
Immunisation status
Although many CYP will report having received some childhood immunisations, they will rarely be able to provide documentation of these. Immunisation schedules vary between countries and vaccine shortages are not infrequent. Catch-up immunisations, including hepatitis B, are recommended for all asylum-seeking CYP as per national guidance22.
Growth and nutrition
While few asylum-seeking children present with acute malnutrition, many are stunted,15 indicating chronic malnutrition secondary to a poor diet prenatally and postnatally15 and subsequent micronutrient deficiencies before and during their journey to the UK. In particular, vitamin D deficiency is prevalent among migrant communities, with one case series reporting a prevalence of 66%.5 Some children are concurrently stunted and obese and therefore at higher risk of ongoing obesity and cardiovascular disease in adulthood. Discussion around diet and food sources is important23 as families may be unfamiliar with local food banks or produce, may have limited facilities for preparing food and be provided with food of poor quality and limited variety. This is especially problematic for families who face prolonged periods in temporary accommodation.
An intergenerational awareness is vital, given the aforementioned importance of an adequate nutritionally and micronutrient rich diet for pregnant women, those wishing to conceive and those who are breast feeding.
Development
There is little in the published literature about developmental delay in migrant children.24 25 The classification and diagnosis of these disorders in this population is additionally challenging due to the paucity of knowledge about the cultural beliefs and perceptions of developmental delay in refugee communities.
Furthermore, the assessment tools have been developed and designed within a Western facing context, in the English language and have not been validated for use in migrant communities.26
These barriers to the early identification of developmental delay have been well described in other migrant groups. One example is the delay in diagnosis of autism spectrum disorders (ASD) in children from black, Asian and ethnic minority groups as compared with white children in Europe and North America.26 27 This has been attributed to racial bias of professionals, barriers to accessing healthcare and cultural misinterpretation of symptoms by both the families and professionals.28 29
Children who have experienced trauma directly may display symptoms such as appearing withdrawn, avoiding eye contact and lacking trust of adults. These symptoms are similar to those of children presenting with a social communication disorder. Failure to recognise these similarities may lead to a further delay in diagnosis. In addition to the direct impact that trauma can have on neurodevelopment,30 it is important to recognise the indirect, intergenerational impact that trauma in family members can have on the development of asylum-seeking children. There is emerging evidence which suggests that highly stressful migration experiences during pregnancy may alter the uterine environment31 leading to epigenetic changes that may increase the risk of ASD.32–34
Potential strategies to improve the identification and diagnosis of social communication disorders and developmental delay in children from migrant communities include the use of: (1) cultural navigators trained to serve as liaisons between their cultural communities and health professionals,35 (2) appropriate developmental screening tools and (3) appropriate interpretation services with visual aids, both for the assessment of the child and to explain the developmental domains to the parents.35 In addition to this, once children are placed in nursery and school, liaising with educational professionals is arguably the best way of identifying, and responding to, any problems in this domain.
Mental health
An awareness of the trauma-informed assessment of mental health status and needs is crucial in this population.36 Specific screening tools such as the Refugee Health Screener 15 have been developed to sensitively detect the range of emotional distress common across refugee groups and are particularly useful in adolescents.37 The Strengths and Difficulties Questionnaire is another paediatric and adolescent one-page screening tool, which is widely used in the UK to identify emotional, behavioural and relationship problems and has been translated into several languages.38–40 It is important to recognise the limitations of these tools as well as their advantages.
UASC endure higher levels of stress compared with accompanied children,41 with associated, long-term mental health repercussions. Prevalence estimates of PTSD among asylum-seeking children have been reported as 11% –75% and of depression from 4 to 47%.40 Deliberate self-harm and suicide attempts were reported in up to 8% of UASC in a central London setting where the overall prevalence of mental health problems was 77%.6 It is important to take time to build trust, as symptoms of trauma may not be apparent initially and disclosure may only occur once they are in a ‘safe haven.’ Many young people find it challenging to talk about their own mental health, particularly as there is significant stigma attached to mental health assessments and diagnoses in some cultures.42 Some resettlement experiences may be triggering of previous trauma, leading to manifestation of symptoms further down the line.43 Pre-existing mental health conditions may become destabilised by poor living conditions, uncertainty and the potential lack of access to previously prescribed medications. Social interventions that provide routine and stability and encourage families and young people to feel part of a community, such as enrolling children into schools, stable and safe housing, opportunities to learn English, voluntary work and knowledge of community support available (eg, through voluntary sector organisations) have a positive effect on mental health42 and should be prioritised.44 45
Safeguarding
In the UK, most UASC will already be known to Children Looked After (CLA) services within Children’s Social Care. In cases where young people aged 17 years and under present prior to engagement with the social care system, a referral to local safeguarding services should be made immediately. Furthermore, all families who are asylum-seeking meet the threshold for Early Help intervention, which is the first tier of support offered by the local authority to families living in challenging circumstances.46 Assessing clinicians should be alert to signs that may indicate a young person may have been trafficked into the UK as these young people remain extremely vulnerable to sexual and criminal exploitation. A sexual health history should be taken in all adolescents and an opportunity provided for CYP to make disclosures about any history of sexual violence. Girls and young women should be asked about female genital mutilation and, if reported, referred to local specialist services.23 Pregnancy testing should be offered to all pubertal females. Adolescents should be asked about tobacco, alcohol and other substance use. There should be awareness of cultural medical practices such as uvulectomy or scarification.47 Health professionals should also be alert to potential specific and more common safeguarding issues for these families. For example, among families seen in a London-based family refugee clinic, domestic violence was reported by 10%.48 It is also important to share with families some of the cultural differences that may trigger safeguarding procedures in the UK, including differences in legal age of marriage and sexual intercourse.
Age dispute
In the event that the topic of age dispute is raised, clinicians should refer to the most recent RCPCH guidance23 which states that ‘it is not possible to accurately predict a child’s age based on physical examination or bone age assessment’. Bone X-rays are not reliable and should not be used for this purpose.
Family context
For children accompanied by family, needs of the parents and siblings should be briefly explored, given the aforementioned intergenerational aspects of refugee health and their long-term impacts. The family should be signposted to sources of support and further assessment where necessary.
Post-assessment and recommendations
At the end of the assessment, a plan should be formulated together with the young person, the child’s family and relevant HCPs.
The plan should be achievable, accompanied by clear explanation, proposed timeline and prioritisation.
Referrals to relevant services in the community should be initiated, and signposting to relevant charities and local food banks. If the CYP does not have an NHS number and/or is not registered with a GP, this should be advocated for. The Refugee Council offers online resources and support to families explaining the NHS services available, how to access these and where to go if urgent treatment is needed.48
Asylum-seeking families are often housed in temporary accommodation for long periods and are at risk of relocation at short notice. It is therefore ideal to provide a paper, patient-held healthcare plan, as well as an electronic version, for all asylum-seeking CYP highlighting outstanding issues and actions. This should be copied to the GP and all relevant HCPs, including the CLA team for UASC. Follow-up appointments should be made prior to discharge and written information provided regarding these.
Conclusion
Asylum-seeking CYP often arrive in their destination countries with complex, interconnecting health and social care needs.
We provide a detailed framework to guide HCPs through a comprehensive assessment of health in newly arrived asylum-seeking CYP. We propose an assessment comprising three stages including careful preplanning, clear documentation and the sharing of a hand-held record that individuals may retain to avoid future retraumatisation and duplication or omission of appropriate interventions.
We emphasise not only the physical and mental health assessment, but also the importance of detailed developmental and safeguarding evaluation.
A trauma-informed, life-cycle and intergenerational approach should be at the heart of every encounter, enabling a safe, comprehensive and holistic assessment. Multidisciplinary team working and utilisation of appropriate networks to share knowledge, experience and skills will also support the delivery of high-quality care using a best-practice approach.
Finally, clinicians and allied health professionals working with asylum-seeking CYP are in a position to be strong advocates for the needs of these underserved communities. We should strive to provide excellent quality care and to improve health and social care systems to ensure equitable access and provision, and optimise outcomes for these vulnerable families.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors NSC, PC, SE, CH and AW wrote the manuscript. SE, CH, AW conceptualised the piece. NL provided significant edits.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Provenance and peer review Commissioned; externally peer reviewed.