Article Text

Abstract
Objective Understanding how paediatric emergency departments (PEDs) across Europe adapted their healthcare pathways in response to COVID-19 will help guide responses to ongoing waves of COVID-19 and potential future pandemics. This study aimed to evaluate service reconfiguration across European PEDs during the initial COVID-19 wave.
Design This cross-sectional survey included 39 PEDs in 17 countries. The online questionnaire captured (1) study site characteristics, (2) departmental changes and (3) pathways for children with acute illness pre and during the first wave of COVID-19 pandemic (January–May 2020). Number of changes to health services, as a percentage of total possible changes encompassed by the survey, was compared with peak national SARS-CoV-2 incidence rates, and for both mixed and standalone paediatric centres.
Results Overall, 97% (n=38) of centres remained open as usual during the pandemic. The capacity of 18 out of 28 (68%) short-stay units decreased; in contrast, 2 units (7%) increased their capacity. In 12 (31%) PEDs, they reported acting as receiving centres for diverted children during the pandemic.
There was minimal change to the availability of paediatric consultant telephone advice services, consultant supervision of juniors or presence of responsible specialists within the PEDs.
There was no relationship between percentage of possible change at each site and the peak national SARS-CoV-2 incidence rate. Mixed paediatric and adult hospitals made 8% of possible changes and standalone paediatric centres made 6% of possible changes (p=0.086).
Conclusion Overall, there was limited change to the organisation or delivery of services across surveyed PEDs during the first wave of the COVID-19 pandemic.
- health services research
- COVID-19
Data availability statement
Data are available upon reasonable request. Data can be made available on reasonable request from the corresponding author Katy Rose at katy.rose2@nhs.net.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
The burden of COVID-19 disease is now known to be lower in the paediatric population compared with the adult population.
Levels of preparedness for a pandemic varied across European paediatric emergency departments (PEDs).
Public health authorities globally issued advice to stream patients into high-risk and low-risk COVID-19 categories.
What this study adds?
The majority of PEDs did not undergo major service change in response to the first wave of the COVID-19 pandemic.
The degree of change in departments was not related to the peak incidence rates of COVID-19 in the country of origin or type of hospital.
This information may help guide responses to ongoing waves of COVID-19 and potential future pandemics.
Introduction/Background
Ever since the first outbreak of SARS-CoV-2 was reported in China, and subsequently the extensive outbreak in Italy in February 2020, the global COVID-19 pandemic has caused significant challenges for healthcare systems and societies at large. One of the few reassuring aspects to emerge as the pandemic progressed is the low infection rates and decreased severity of disease in children compared with adults.1–4 The multisystem inflammatory syndrome in children has presented as a novel and severe complication but case numbers remain extremely low comparative to the adult acute and chronic disease burden.5–8 Numbers of children attending the paediatric emergency departments (PEDs) with most other types of acute illness have also been reported to have fallen drastically.9–13
Globally, public health bodies recognised the need to separate patients high risk for COVID-19 and low risk for COVID-19 presenting to healthcare services; by 15 March 2020, over 75% of surveyed centres in Europe had a pre-triage process to achieve this.14–16 In the USA, there were country wide efforts to consolidate paediatric inpatient and community care to specialised centres.17 In Europe, there was no formal coordinated strategy for the restructuring of paediatric patient flow.18 19 The substantial differences in emergency department (ED) preparedness, surge capacity and management of paediatric suspected COVID-19 cases between countries were highlighted in the early stages of the pandemic.16
Currently, insights into the European approach to organising healthcare for children with acute illness in response to infectious pandemic and global disasters are limited. Better understanding of PED responses beyond divisions of patients by risk category will help our response to future disasters. This multinational, cross-sectional European survey aimed to understand the types of changes in paediatric emergency care delivery, which were implemented in response to the first wave of COVID-19.
Methods
Study design
This survey was undertaken as part of the ‘Epidemiology, severity and outcomes of children presenting to emergency departments across Europe during the SARS-CoV-2 pandemic’ (EPISODES) study. Sites were selected directly from the Research in European Paediatric Medicine (REPEM) and European Society of Emergency Medicine (EUSEM) networks, or indirectly via national representatives of the REPEM network and following engagement with the earlier work of Bressan et al.16 Unlike this earlier work, centres could only be included if they could rapidly meet these criteria: (1) data sharing agreement in place, (2) ethics approval, (3) aggregated data available on ED presentation via electronic health records.
Initially, 53 hospitals in 20 European countries expressed interest in participation; within these restrictions, 39 hospitals from 17 European countries were able to participate in the study. The final EPISODE cohort included an additional centre whom did not enter the study early enough to contribute to this piece of work and this cohort includes one centre whom unfortunately could not continue contributing to the wider study. Ethics approval was obtained by the ethics committee or institutional review board at each participating site (online supplemental appendix 1). The survey was distributed online via the Research Electronic Data Capture (REDCap) platform between 6 October 2020 and 6 February 202120 among the EPISODES study sites (online supplemental appendix 2). Each participating institution provided one response, completed by one of the local site investigators.
Supplemental material
Supplemental material
No patient identifiable data were used in this survey.
Survey development
The survey was developed according to best practice on survey methodology and reviewed iteratively by the study team, with input from clinical experts and the EPISODES Steering Committee, considering the reporting guidelines for Internet E-Surveys.21 Survey domains were chosen based on expert consensus and were piloted prior to full use; questions were, in part, based on previous similar study designs.16 22–24
We asked site leads for the EPISODES study to complete the survey themselves or delegate to the most appropriate person within the ED. All respondents were experienced paediatric or emergency medicine trained physicians with experience of working in and/or leading their local (paediatric) ED.
The first part of the survey contained questions relating to baseline hospital demographics and working models such as triage tools, paediatric intensive care unit (PICU) support and the length of ED stay limitations. The study considered the time frame prior to February 2020 as pre-COVID-19; the second section of the survey included questions relating to changes to patient pathways and services triggered by the pandemic outbreak.
Response options included 5-point Likert scales, multiple selections, single answers or free text. Respondents were encouraged to include additional details in free text if the standardised questions did not fully encompass the local changes, or where wider regional health service organisation needed explanation. These will be highlighted in case examples where relevant. The full survey is available in online supplemental appendix 2; it includes questions pertaining to therapeutics which do not serve to inform this study. Clarification and expansion of answers was sought through email and video correspondence with the study site leads if necessary. Study site leads were either departmental clinical leads or nominated clinical deputies.
The survey covered domains that represented 37 possible points of change in provision of care for sites without a short stay unit (20 pertaining to service provision and 17 to patient pathways) and 38 possible points of change for those that did (21 service provision and 17 patient pathways). These questions are highlighted yellow in the online supplemental appendix 2.
Analyses
Descriptive results are presented as numbers and percentages for categorical variables, and means or medians with SD or IQR for continuous variables as appropriate.
We compared the percentage and number of changes in provision of care at each site to (1) the SARS-CoV-2 disease incidence as per the all age, peak national 14-day COVID-19 infection rate (per 100 000) as per European Centre for Disease Prevention and Control (ECDC) for each country,25 and (2) hospital type: mixed adult and paediatric hospitals versus standalone paediatric hospitals. Each point of change was assigned equal weight, with each site being assigned a site-specific percentage of change. As the variance of count of changes was higher than the mean, we used a negative binomial regression to determine associations between count of changes and peak infection rates and hospital type. We considered univariable associations, and associations adjusted for other key factors of the hospital and local community care. The variables considered were type of ED; urban or rural setting; whether the hospital is a major trauma centre; the number of beds; whether patients had access to primary care 24hours and whether the hospital had a PICU. Significance was defined as p<0.05.
Analyses were performed using R V.4.0.3.26
Results
Baseline demographics
All 39 sites responded to the survey questions; 34 (87%) sites provide tertiary paediatric care with 16 PEDs (42%) in standalone paediatric hospitals. Further baseline hospital demographics are presented in table 1 and online supplemental table 1.
Supplemental material
Demographics and hospital characteristics
All departments served areas with in-hours primary care facilities, 21 departments (54%) had weekend and evening services with 17 (44%) located in areas with night time availability of primary care. Sources of referral varied with all departments accepting referrals from emergency services (e.g. ambulances) but only 5 (13%) centres accepting referrals from all sources (online supplemental table 2).
No ED had a paediatric upper age limit beyond a young person’s 19th birthday (online supplemental table 3).
COVID-19 changes
Overall patterns
All but one of the surveyed departments remained open for all children. Most (23, 59%) departments reported that other regional hospitals remained open as usual; 12 (31%) departments reported acting as receiving centres for diverted children during the pandemic (table 2). A single centre reported now being the sole receiving centre for paediatric patients and five(13%) with partial redirection of children from other centres. An additional three (8%) participating centres had been the only hospital with acute paediatric services within their region since 2018; this precluded any further service consolidation.
Diverted paediatric patient groups during COVID-19 time period
Prior to the pandemic, 28 of the 39 (72%) PEDs had the availability of a short stay unit; during the pandemic, 18 of these 28 departments reported changes to availability, with 2 (7%) reporting increased availability, 11 (39%) reporting decreased availability and 5 (18%) closing completely (online supplemental table 3).
Most hospitals (32, 82%) had no prehospital (primary care, emergency service or front door) streaming of patients with suspected COVID-19 away from their department to another acute and emergency care provider in the region. Seven (18%) had primary care or emergency service streaming of patients with COVID-19. Four (10%) departments operated streaming pathways at the ED front door from which patients with suspected COVID-19 were directed to alternative hospitals (online supplemental table 4).
Unique centre changes
A single department in Dublin, Ireland, closed to paediatric patients during the pandemic (13 March–31 August 2020). Patients were diverted to the two other PEDs within Dublin and staff were redeployed locally or to the other departments based on skill sets and staff personal preference. Another ED in the Netherlands did not formally close to ED paediatric attendances but shifted to a model where most patients triaged to be seen directly on the paediatric ward rather than in the ED; notable exceptions were major trauma, critically unstable children and children in need of multiple specialty review. One department in Amadora, Portugal, closed for 2 weeks at the peak of the pandemic owing to COVID-19 infection levels in staff. In Szekesfehervar, Hungary, and Vienna, Austria, the departments diverted children with suspected COVID-19 to alternative hospitals. In Ljubljana, Slovenia, where children in PED are usually seen exclusively after primary care referral, a screening mechanism was introduced so that ‘for every child that was referred to our ED, the primary paediatricians had to have a telephone consultation with one of our paediatricians first’. In addition, all paediatric COVID-19 suspected cases in Slovenia were diverted to their infectious disease hospital. In Rome, Italy, the ED was open to all children but once determined to be high risk for COVID-19 and stable, they were transferred to a single designated hospital (Bambino Jesu, Rome).
Changes to services
Only two PEDs increased their age limit during the pandemic, one from the 16th birthday to the 18th birthday and the other from the 17th birthday to the 19th birthday.
Prior to the pandemic, 22 (56%) departments provided a consultant advice telephone line for general practitioners; this was continued in all cases with an additional 2 departments starting this service so that 24 (62%) centres were providing this during the pandemic (figure 1). In all the departments which remained open during the pandemic, daytime direct consultant cover remained constant (97% of departments). Consultant cover out of hours (OOH) and at night underwent minimal change (online supplemental figure 1). There was little change in responsible teams in the PED (online supplemental figure 1).

Consultant advice line provision.
Diversion of children with underlying comorbidity occurred to some extent in 16 (42%) departments prior to the pandemic and 13 (34%) during. This was implemented as a new pathway in two departments (5%) but five (13%) stopped such pathways (online supplemental table 3).
Changes and burden of COVID-19
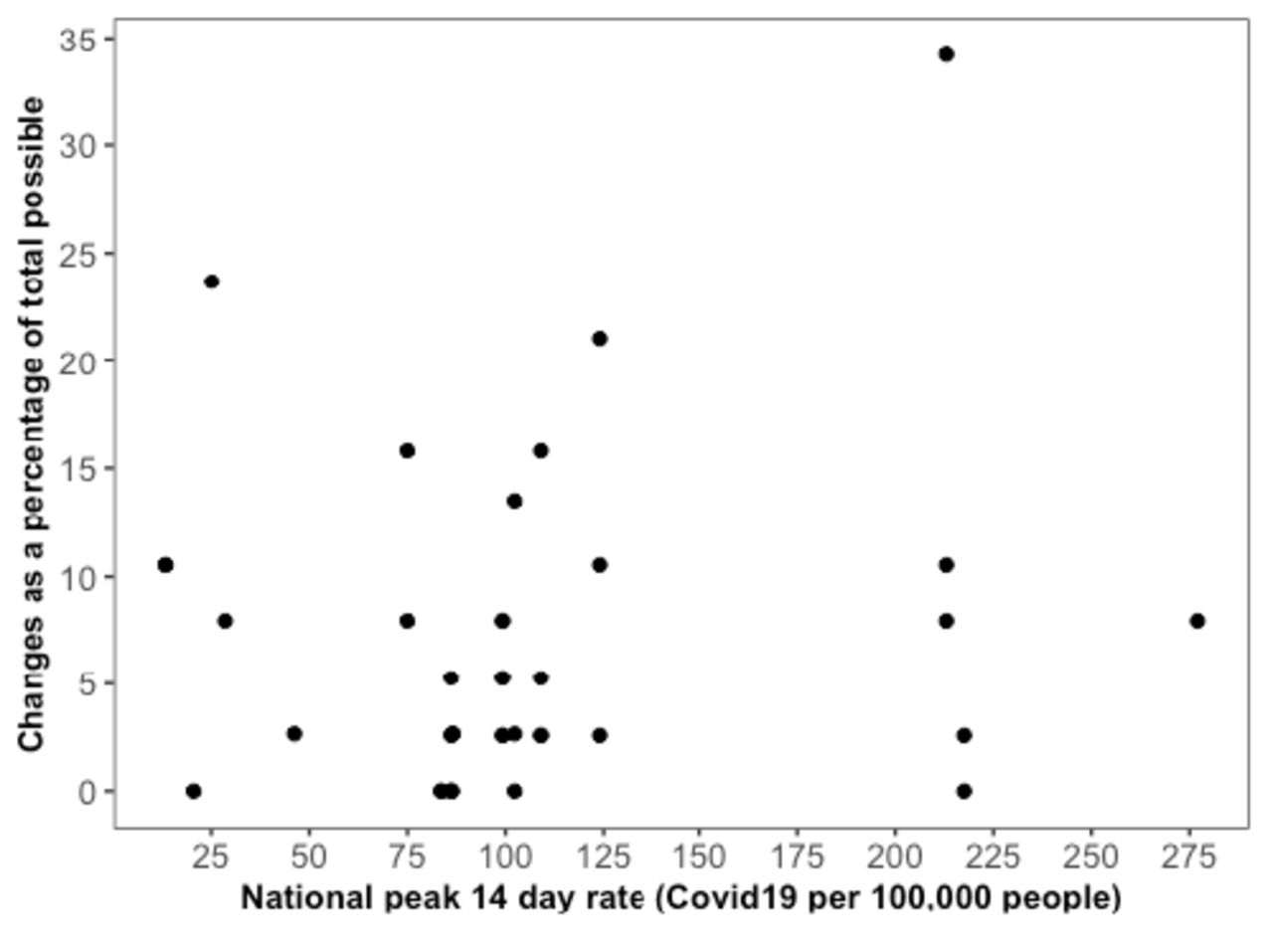
Figure 2 illustrates the average percentage change across countries and figure 3 shows the relationship between percentage change and peak rate of COVID-19, these are both displayed by specific study site in online supplemental figure 2. We found that mixed hospitals (n=22) made 8% of possible changes and standalone centres (n=16) made 6% of possible changes.
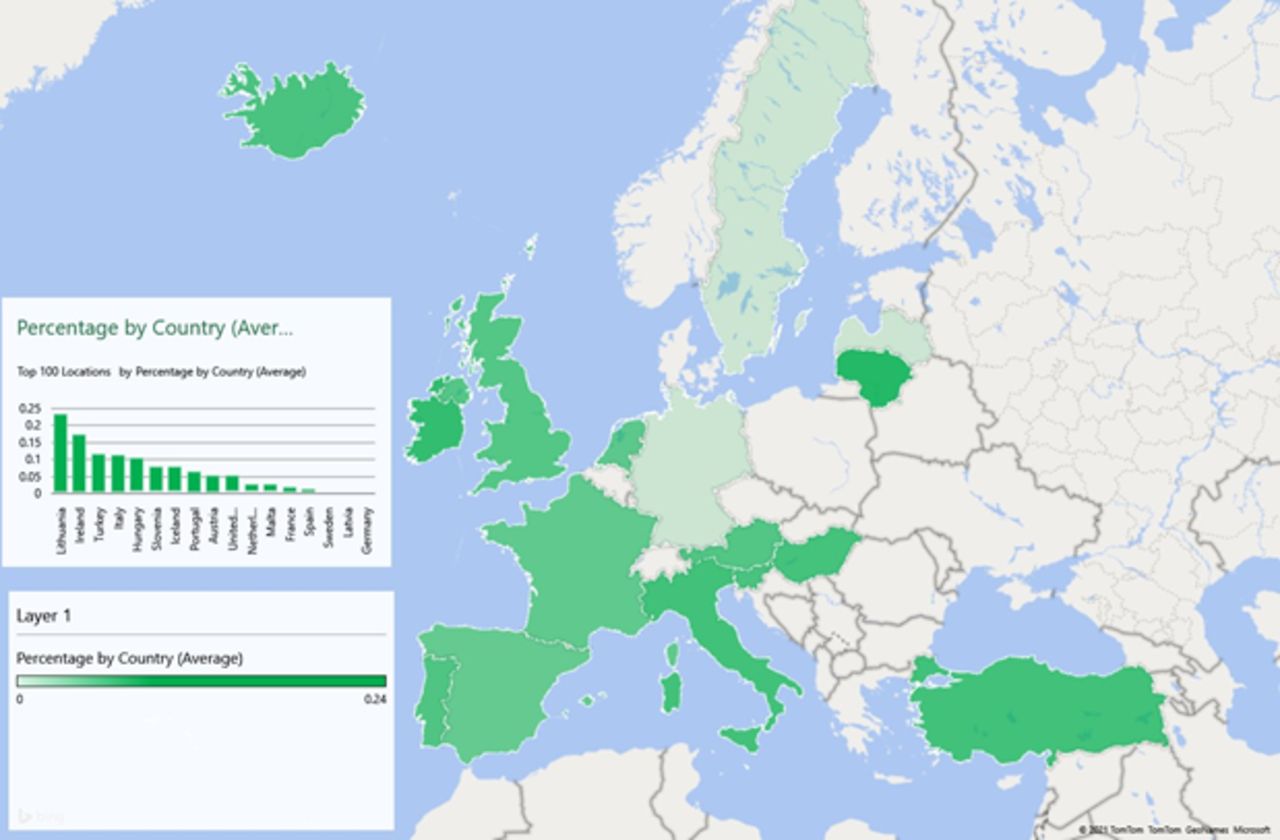
Average percentage of change by country.
{kind=link}
{kind=link}
{kind=link}
Percentage changes for each department compared with peak 14-day COVID-19 incidence rate. Departments with a short stay unit had a potential for 38 changes where departments without a short stay unit had a potential for 37 changes. All potential changes were ascribed equal weights. The peak 14-day COVID-19 incidence rate is as per the European Centre for Disease Prevention and Control figures.
Univariable analysis showed no significant relationship between frequency of changes and national peak incidence rates nor type of hospital. After adjusting for hospital and primary care factors, higher number of changes was significantly associated with mixed adult and paediatric hospital with most paediatric subspecialities (n=14) when compared with paediatric standalone hospitals (n=16) (online supplemental table 5).
Discussion
The results of our cross-sectional survey among 39 sites in 17 European countries show a low level of change in provision of care in these PEDs in Europe during the first wave of the COVID-19 pandemic. Some PEDs implemented large-scale changes, but these were a minority, and overall our findings showed a service delivery with a largely ‘business as usual’ approach. There were slightly more changes to regional healthcare pathways for mixed adult and paediatric hospitals compared with standalone paediatric hospitals. Percentage change appeared to be unaffected by the national peak SARS-CoV-2 rates.
Healthcare structure and service delivery across the included countries all have a backbone of universal access, but otherwise often differ greatly in how the health system is organised.27–30 This study shows that across these systems, vast changes to PED were not implemented in order to manage the care of acutely unwell children during the pandemic regardless of how a healthcare system is structured more widely.
Others have highlighted changes which encompassed the necessity to separate high-risk and low-risk COVID-19 streams at the ED front door.16 31 This was also echoed by many of our respondents; however, only a few departments redirected children to other hospitals at the point of front-door access. Earlier work suggested that hospitals achieved this separation within their pre-existing local departments through the use of physical or staff level divides.16
Once fully adjusted, our data support that mixed children’s and adults’ centres with most paediatric subspecialities underwent proportionally higher changes than standalone units. This would perhaps be expected, given increased demands from adult services in large centers coping with the high numbers, and acuity, of patients with COVID-19. However, regional consolidation of services to dedicated paediatric centres was uncommon with only 12 centres having any kind of diversion in place. This means that, although we have a selected sample, there is no immediate evidence that the regional hospitals streamed patients away to other sites. This pattern was not dissimilar to that reported in America, where despite suggestion from the Children’s Hospitals Association (CHA) to consolidate services, very few hospitals reported doing so.17 31
In contrast to the USA experience, there was almost no change to staffing in terms of responsible clinicians or consultant cover within our centres despite the decrease in patient numbers. This is unlikely to represent fewer specialist doctors working within the US hospital system, given an arguably more established PEM training route.32 33 It is also not explained by the proportion of standalone paediatric departments, which were similar to the US representation,31 from which redeployment of staff may not be feasible. It is possible to hypothesise that incidence rates could affect changes; either higher incidence requiring more change or lower incidence allowing more time to make changes. However, looking at our data national SARS-CoV-2 peak incidence rates were not related to the extent of reconfiguration. Further exploration to understand the reasons behind changes, or lack of changes, across departments would be helpful to understand these patterns. Our survey used consultant cover as a proxy measure for staffing generally; if junior staffing was significantly changed, it is expected the consultant staffing would have to change to reflect this, explicit exploration of this may be useful in future work.
A consistent pattern of change was that most units with a short stay unit restricted these services in some capacity. It remains unclear if this was driven primarily by the decrease in paediatric patient numbers, or in response to the need for more adult footprint within departments, or both.
Alongside the low burden of COVID-related serious disease in children, PEDs globally also saw a steep decline in paediatric attendance overall.9 12 34 35 In the pandemic, the quantity of ‘unknowns’ has been vast, and many systems have responded in semi-reactionary manners, perhaps explaining the larger changes made in mixed centres. The low patient volumes may have meant that most PEDs did not require significant changes which adult ED may have undergone in order to adequately react to the situation as it unfolded across the globe.36–38
The requirement to maintain a safe level of emergency paediatric care may also have seen smaller changes to the ED working than primary care, community, inpatient and outpatient paediatric services. Changes in the wider models of healthcare around children and young people may have contributed to the PED model remaining constant. Although referral pathways into the PED did not appear to change, there were extensive changes elsewhere in paediatric care which may have impacted the ED. Encouragingly, new work is continually emerging to add to understanding the full effects of the pandemic on children and young people’s healthcare services.39–41 This would be important to understanding whether, if in future pandemics, children remain minimally affected could PEDs seek to make wider changes to allow more assistance to our adult colleagues and patients?
Our results should be interpreted in the lights of study limitations. First, the survey was primarily designed to inform the response of PEDs during the first wave of the COVID-19 pandemic in the context of the EPISODES study. As discussed, wide changes in the paediatric healthcare system have not been thoroughly captured. In addition, the subset of European centres included may not be representative of all the European PEDs. The majority of participating sites were tertiary, specialised PEDs. Hence, our results might not necessarily reflect changes made in general or smaller hospitals. However, the majority of sites were not receiving diverted paediatric patients from regional hospitals, which suggests that major restructuring was not being experienced more widely.
Second, the correlation of change to all-age and national incidence rates is a reflection of an expected overall burden to entire healthcare systems and may not be representative of the paediatric specific experience.
Third, we developed an approach to quantify change which has not been validated. In this approach, all changes have been ascribed equal weights. Some may be considered to have a greater impact on direct care in the ED, some to have more system wide effects. In addition, this survey did not reflect changes over time instead asking departments to reflect on total changes made some months after the end of the first wave of COVID-19 in Europe. Refining this approach could be considered in further similar studies surrounding care delivery in future pandemic response.
Finally, this study did not consider the different funding structures behind hospitals across Europe which may have changed how services could or could not be altered. However, given that largely there was minimal change across a broad range of countries, it seems this was not likely to have been a significant factor. Given the earlier work by Bressan et al, and the existing length of our survey, we did not explore further how hospitals achieved the division into high-risk and low-risk COVID-19 groups; additional learning may be possible in this area.
Similar to earlier work in America and Europe, many respondents commented on low paediatric patient volume being the most apparent change.16 31 Further work to understand this impact, as well as disease type and severity, is ongoing as part of the EPISODE study group work; preliminary data echo significant reduction in patient volume.
Conclusion
Overall, there was little change to service organisation or delivery across these PEDs during the first wave of the COVID-19 pandemic. Mixed centres appeared to have made more changes but patterns to these changes are not apparent. A few centres underwent greater degrees of reorganisation mainly in consolidation of services which have the potential to be replicated by others in future pandemic responses. Although children remained largely unaffected by this pandemic, there is scope for learning from centres who made larger scale changes in thinking about future responses. It is possible that in future waves of this, or similar pandemics, PEDs could make wider changes if health systems required this.
Data availability statement
Data are available upon reasonable request. Data can be made available on reasonable request from the corresponding author Katy Rose at katy.rose2@nhs.net.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
Celia Nekrouf (Paediatric Emergency Department, Hopital Universitaire Robert-Debre, Paris, France); Marcello Covino (Emergency Department, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy); Benita Lund (Medical Secretary; Paediatric Emergency Department, Sachs’ Children and Youth Hospital, Stockholm, Sweden); Izabella Lottiger (Paediatric Emergency department, Astrid Lindgren Children Hospital, Stockholm, Sweden); Sharna Crosdale (Contracts office; Imperial College London, UK); Sarah Sheedy (Research nurse; Emergency Department, Bristol Royal Hospital for Children, Bristol, UK); James Allbones (Information & Performance Analyst; Birmingham Women’s and Children’s NHS Foundation Trust, UK), William Jones (University Hospitals of Leicester NHS Trust, UK); Frazer Snowdon and Matthew Ryan (Paediatric emergency department, Alder Hey Children’s NHS Foundation Trust, Liverpool, UK), Carlos Saiz-Hernando (IT analyst; Department of Medical Documentation, Cruces University Hospital, Bilbao, Spain); Ellen Barry (research nurse; National Children’s Research Centre, Dublin, Ireland); Ernst Eigenbauer (data analyst) and Katharina Lieb (medical student; Department of Paediatrics and Adolescent Medicine, Vienna, Austria); Sanne Vrijland (medical student; Erasmus MC – Sophia Children’s hospital, Rotterdam, The Netherlands); Catarina Cordeiro (Paediatric Emergency Service, Hospital Pediátrico, Centro Hospitalar e Universitário de Coimbra, Portugal); Mark Camenzuli (Senior systems administrator; Mater Dei Hospital, Malta); Sandra Distefano (Clinical Performance Unit, Mater Dei Hospital, Malta); Karin Kittl-Mitteregger (HIS Management and Clinical Processes, Paracelsus Medical University, Salzburg, Austria).
References
Footnotes
Twitter @rgnijman
Collaborators Alexis Rybak, alexis.rybak@aphp.fr, 0000-0002-2898-3710, Paediatric Emergency Department, Hopital Universitaire Robert-Debre, Paris, France; Ana Sofia Simões, anasofiasimoes@chuc.min-saude.pt, 0000-0001-8443-0689, Pediatric Emergency Service, Hospital Pediátrico, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; Antonio Chiaretti, antonio.chiaretti@unicatt.it, 0000-0002-9971-1640, Department of Woman and Child Health and Public Health, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy; Asgeir Haraldsson, asgeir@landspitali.is, Children's Hospital, Barnaspitali Hringsins, Reykjavik, Iceland; Borja Gomez, borja.gomezcortes@osakidetza.eus, 0000-0001-6542-4494, Paediatric Emergency Department, Cruces University Hospital, Barakaldo, Spain; Biocruces Bizkaia Health Research Institute, Cruces University Hospital, Barakaldo, Spain; Camille Aupiais, camille.aupiais@aphp.fr, 0000-0001-7482-0405, Université Paris 13, Sorbonne Paris cité, Assistance Publique-Hôpitaux de Paris, Jean Verdier Hospital, Pediatric Emergency Departement, Bondy, France; Institut National de la Santé et de la Recherche Médicale UMR 1123, ECEVE, Paris, France; Caner Turan, canertrn@yahoo.com, 0000-0002-6375-9829, Department of Pediatrics, Division of Emergency Medicine, Mersin City Training and Research Hospital, Toroslar, Mersin, Turkey; Christoph Zurl, christoph.zurl@medunigraz.at, 0000-0003-0623-0360, Medical University of Graz, Department of General Paediatrics, Graz, Austria; Clarissa Barber, clarissa.barber@uhbw.nhs.uk, 0000-0001-8462-618X, Paediatric emergency department, University Hospitals Bristol NHS Foundation Trust, Bristol, UK; Corinne Vasilico, c.vasilico@salk.at, 0000-0001-8911-1097, Department of Pediatrics, Paracelsus Medical University, Salzburg, Austria; Daniel Weghuber, d.weghuber@salk.at, 0000-0002-4389-0379, Department of Pediatrics, Paracelsus Medical University, Salzburg, Austria; Daniela Kohlfuerst, daniela.kohlfuerst@medunigraz.at, 0000-0002-1188-9525, Medical University of Graz, Department of General Paediatrics, Graz, Austria; Danielle Rose, danielle.rose19@imperial.ac.uk, Global Digital Health Unit, School of Public Health, Imperial College London, UK; Dorine Borensztajn, dm.borensztajn@nwz.nl, 0000-0002-2437-0757, Department of Paediatrics, NoordWest Ziekenhuisgroep, Alkmaar, Netherlands; Esra Akyüz Özkan, uzdresra@gmail.com, 0000-0001-9412-8010, Paediatric Emergeny Department, Ondokuz Mayıs University, Samsun, Turkey; Fiona Leonard, fiona.leonard@olchc.ie, Paediatric Emergency Department, Children's Health Ireland at Crumlin, Ireland; Florian Hey, Florian.Hey@med.uni-muenchen.de, 0000-0001-6183-5798, Paediatric emergency department, Dr. von Hauner Children’s Hospital, Ludwig-Maximilians-University Munich, Munich, Germany; Florian Hoffman, Florian.Hoffmann@med.uni-muenchen.de, 0000-0002-2713-2455, Paediatric emergency department, Dr. von Hauner Children’s Hospital, Ludwig-Maximilians-University Munich, Munich, Germany; Francisca Saraiva, francisca.saraiva@hff.min-saude.pt, 000-0002-6082-7160, Departamento da Criança e do Jovem- Urgencia Pediatrica, Hospital Prof. Doutor Fernando da Fonseca, Amadora, Portugal; Gábor Simon, gsimondr@hotmail.com, Paediatric Emergency Department, Szent Gyorgy University Teaching Hospital of Fejer County, Szekesfehervar, Hungary; Inês Mascarenhas, maria.i.mascarenhas@hff.min-saude.pt, 0000-0002-5463-8857, Departamento da Criança e do Jovem- Urgencia Pediatrica, Hospital Prof. Doutor Fernando da Fonseca, Amadora, Portugal; João Viana, joao.a.viana@gmail.com, Centro Hospitalar e Universitário de São João, Porto, Portugal; John Jensen, John.Jensen@alderhey.nhs.uk, 0000-0003-2571-0263, Paediatric emergency department, Alder Hey Children's NHS Foundation Trust, Liverpool, UK; Jonas Thüminger, j.thueminger@salk.at, 0000-0002-0191-7561, Department of Paediatric and Adolescent Surgery, Paracelsus Medical University, Salzburg, Austria;Julia Lischka, julia.lischka@meduniwien.ac.at, 0000-0002-7047-3829, Clinical Division of Paediatric Pulmonology, Allergology and Endocrinology, Department of Paediatrics and Adolescent Medicine, Comprehensive Centre for Paediatrics, Medical University of Vienna, Vienna, Austria; Katarina Vincek, keti.vincek@gmail.com, University Medical Centre Ljubljana, Univerzitetni Klinični Center, Department of Infectious Diseases, Ljubljana, Slovenia; Laszlo Fodor, fodordr@gmail.com, 0000-0002-4984-4058, Paediatric Emergency Department, Szent Gyorgy University Teaching Hospital of Fejer County, Szekesfehervar, Hungary; Lia Mano, lia.costa.mano@gmail.com, 0000-0003-1825-9750, Hospital Dona Estefania, Centro Hospitalar de Lisboa Central, Portugal; Lina Jankauskaite, lin.jankauskaite@gmail.com, Hospital of Lithuanian University of Health Sciences Kauno Klinikos, Lithuania; Malin Ryd Rinder, malin.ryd-rinder@sll.se, 0000-0002-2947-4117, Paediatric emergency department, Astrid Lindgrens Children's hospital, Karolinska University, Sweden; Mark Lyttle, mdlyttle77@gmail.com, 0000-0002-8634-7210, Paediatric emergency department, University Hospitals Bristol NHS Foundation Trust, Bristol, UK; Matthias Schaffert, m.schaffert@salk.at, 0000-0003-2594-8888, Department of Paediatric and Adolescent Surgery, Paracelsus Medical University, Salzburg, Austria; Merve Havan, merve-havan@outlook.com, 0000-0003-3431-7906, Department of Pediatrics, Division of Emergency Medicine, Mersin City Training and Research Hospital, Toroslar, Mersin, Turkey; Michael Barrett, Michael.Barrett@olchc.ie, 0000-0003-1775-8347, Paediatric Emergency Department, Children's Health Ireland at Crumlin, Ireland; Michael Bennett, michael.bennett@tuh.ie, Paediatric Emergency Department, Children's Health Ireland at Tallaght, Ireland; Mojca Kolnik, mojca.kolnik@kclj.si, 0000-0003-4194-7295, University Medical Centre Ljubljana, Univerzitetni Klinični Center, Department of Infectious Diseases, Ljubljana, Slovenia; Naomi Lin, naomi.lin@nhs.net, 0000-0002-1652-3055, Department of Paediatric Emergency Medicine, Division of Medicine, St. Mary’s hospital; Imperial College NHS Healthcare Trust,London, UK; Nuno Serra de Almeida, nuno_almeida_75@msn.com, 0000-0003-2230-6214, Pediatric Emergency Service, Hospital Pediátrico, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; Orkun Aydın, orkunaydin.89@gmail.com, 0000-0002-3155-540X, Division of Pediatric Emergency Medicine, Department of Pediatrics, Hacettepe University School of Medicine, Ankara, Turkey; Ozlem Teksam, ozlemt@hacettepe.edu.tr, 0000-0003-1856-0500, Division of Pediatric Emergency Medicine, Department of Pediatrics, Hacettepe University School of Medicine, Ankara, Turkey; Paddy Fitzpatrick, patrick.fitzpatrick@cuh.ie, Paediatric Emergency Department, Children's Health Ireland at Temple Street, Ireland; Patrícia Mação, patriciamacao@chuc.min-saude.pt, 0000-0002-1076-806X, Pediatric Emergency Service, Hospital Pediátrico, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; University Clinic of Pediatrics, Faculty of Medicine, University of Coimbra, Portugal; Petra Salamon, salamon.petra.zsofia@gmail.com, Paediatric Emergency Department, Heim Pal National Paediatric Institute; Roberto Velasco, robertovelascozuniga@gmail.com, 0000-0003-0073-2650, Pediatric emergency unit, Hospital Universitario Río Hortega, Valladolid, Spain; Rohan Mongru, rohan.mongru13@imperial.ac.uk, Section of Paediatric Infectious Diseases, Department of Infectious Diseases, Faculty of Medicine, Imperial College London, UK; Romain Basmaci, romain.basmaci@aphp.fr, 0000-0002-5277-0002, Paediatric Emergency Department, Louis Mourier Hospital, Colombes, France; Romain Guedj, romain.guedj@aphp.fr, Paediatric Emergency Department, Armand Trousseau Hospital, Paris, France; Rosa Morello, rosa.morello91@gmail.com, Department of Woman and Child Health and Public Health, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy; Samuel Rhedin, samuel.rhedin@ki.se, 0000-0001-5798-2875, Paediatric emergency department, Sachs Children and Youth Hospital, Karolinska University, Sweden; Sandra Soares Cardoso, sandraacardosoo@gmail.com, 0000-0002-0362-5650, Pediatric Department, Centro Hospitalar Tondela-Viseu, Viseu, Portugal; Shrouk Messahel, Shrouk@doctors.org.uk, Paediatric emergency department, Alder Hey Children's NHS Foundation Trust, Liverpool, UK; Sofia Rapti, sofia.rapti@gstt.nhs.uk, Department of paediatric emergency medicine, St. Thomas' hopital, Guy's and St. Thomas' NHS Foundation Trust, London, UK; Sofia Reis, reis.carlasofia@gmail.com, 0000-0002-3667-9241, Pediatric Department, Centro Hospitalar Tondela-Viseu, Viseu, Portugal; Sonia Andrade Santos, soniaandradesantos@usal.es, 0000-0002-8085-641X, Pediatric Department, Centro Hospitalar Tondela-Viseu, Viseu, Portugal; Stuart Hartshorn, stuart.hartshorn@nhs.net, 0000-0003-0419-1564, Paediatric emergency department, Birmingham women's and children's NHS Foundation Trust, Birmingham, UK; Birmingham Clinical Trials Unit, Institute of Applied Health Research, University of Birmingham, Birmingham, UK; Susana Castanhinha, susanacastanhinha@gmail.com, 0000-0003-0762-7730, Hospital Dona Estefania, Centro Hospitalar de Lisboa Central, Portugal; Susanne Greber-Platzer, susanne.greber-platzer@meduniwien.ac.at, 0000-0002-3706-8370, Clinical Division of Paediatric Pulmonology, Allergology and Endocrinology, Department of Paediatrics and Adolescent Medicine, Comprehensive Centre for Paediatrics, Medical University of Vienna, Vienna, Austria; Sylvester Gomes, sylvester.gomes@gstt.nhs.uk, Department of paediatric emergency medicine, St. Thomas' hopital, Guy's and St. Thomas' NHS Foundation Trust, London, UK; Thibault de Groc, thibault.degroc@aphp.fr, General Paediatrics and Paediatric Emergency Department, Louis Mourier Hospital, Colombes, France; Tobias Alfven, tobias.alfven@ki.se, 0000-0002-2328-3512, Paediatric emergency department, Sachs Children and Youth Hospital, Karolinska University, Sweden; Urdur Jonsdottir, Children's Hospital, Barnaspitali Hringsins, Reykjavik, Iceland; Valtýr Stefánsson Thors, valtyr@landspitali.is, 0000-0002-0976-9604, Children's Hospital, Barnaspitali Hringsins, Reykjavik, Iceland; Vanda Anacleto, vanda.a.bento@hff.min-saude.pt, 0000-0001-7896-9768, Departamento da Criança e do Jovem- Urgencia Pediatrica, Hospital Prof. Doutor Fernando da Fonseca, Amadora, Portugal; Vanessa Gorito, vanessaoliveiragorito@gmail.com, Centro Hospitalar e Universitário de São João, Porto, Portugal; Vytenis Masillonis, masilionisvytenis@gmail.com, Hospital of Lithuanian University of Health Sciences Kauno Klinikos, Lithuania; Zanda Pučuka, zanda.pucuka@bkus.lv, 0000-0002-6070-3563, Paediatric emergency department, Children's Clinical University Hospital, Riga Stradins University, Riga, Latvia.
Contributors The PI for the EPISODES study is RN. RN conceived and planned the study and worked alongside the EPISODE Steering Committee to establish the protocol and data collection for this study. KR, RN and SB were responsible for data analysis and interpretation with supervision from KH. KR was responsible for leading writing of this manuscript with SB, RN, KH and LT forming the writing group. KR acts as the guarantor for this study. All authors, as part of the EPISODE Steering and study group, provided critical feedback and helped shape the research, analysis and manuscript.
Funding KR is funded by the University College London NHS Foundation Trust as part of a Senior Clinical Fellowship role, RN is funded for his research via NIHR ACL award (CL-2018-21-007). Imperial College London is the main research sponsor of this study.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.