Article Text

Abstract
Objective To compare outcome after less invasive surfactant administration (LISA) and primary endotracheal intubation (non-LISA) in infants born before gestational age (GA) 28 weeks.
Setting All neonatal intensive care units (NICUs) in Norway during 2012–2018.
Methods Defined population-based data were prospectively entered into a national registry. We compared LISA infants with all non-LISA infants and with non-LISA infants who received surfactant following intubation. We used propensity score (PS) matching to identify non-LISA infants who were similar regarding potential confounders.
Main outcome variables Rate and duration of mechanical ventilation (MV), survival, neurological and gastrointestinal morbidity, and need of supplemental oxygen or positive pressure respiratory support at postmenstrual age (PMA) 36 and 40 weeks.
Results We restricted analyses to GA 25–27 weeks (n=843, 26% LISA) because LISA was rarely used at lower GAs. There was no significant association between NICUs regarding proportions treated with LISA and proportions receiving MV. In the PS-matched datasets, fewer LISA infants received MV (61% vs 78%, p<0.001), and they had fewer days on MV (mean difference 4.1, 95% CI 0.0 to 8.2 days) and lower mortality at PMA 40 weeks (absolute difference 6%, p=0.06) compared with all the non-LISA infants, but only a lower rate of MV (64% vs 97%, p<0.001) and fewer days on MV (mean difference 5.8, 95% CI 0.6 to 10.9 days) compared with non-LISA infants who received surfactant after intubation.
Conclusion LISA reduced the rate and duration of MV but had no other clear benefits.
- neonatology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Relevant data are included in text. Data files may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Less invasive surfactant administration (LISA) is generally recommended over primary endotracheal intubation and subsequent surfactant administration in infants with respiratory distress syndrome.
The scientific basis for recommending LISA is weak.
What this study adds
LISA was rarely used before 25 weeks’ gestational age (GA).
For infants with GA 25–27 weeks, the benefits of LISA were a moderately reduced need for and duration of mechanical ventilation (MV).
Variation between neonatal intensive care unit (NICUs) in use of LISA and use of MV may indicate that NICU routines are as important as LISA versus non-LISA strategy.
How this study might affect research, practice and/or policy
Potential benefits and risks of LISA in the more immature infants need to be investigated.
Introduction
The 2019 European Consensus Guidelines on the management of respiratory distress syndrome (RDS) recommends less invasive surfactant administration (LISA) as the preferred mode of surfactant administration in spontaneously breathing infants with respiratory distress.1 The method implies the administration of surfactant through a thin catheter, which is briefly placed in the trachea under direct laryngoscopy while the infant is on continuous positive airway pressure (CPAP). The guideline is based on interpretations of randomised clinical trials (RCTs) and meta-analyses suggesting that LISA reduces the need of endotracheal intubation and mechanical ventilation (MV) and is associated with lower risks of death and bronchopulmonary dysplasia (BPD), as compared with administration of surfactant after intubation and MV.1 The recommendation was considered weak because some of the background studies were open to bias.1
The later updated Cochrane review confirmed the findings reported in the European guidelines and also found that LISA reduced the risk of severe intracranial haemorrhage (ICH).2 However, the Cochrane authors expressed concerns that the meta-analysis did not allow reliable subgroup analyses and that the number of infants with gestational age (GA) less than 28 weeks was limited.2 A recent large multicentre RCT of infants with GA 25–28 weeks did not find a significant reduction in the composite outcome of death and BPD when using minimally invasive surfactant therapy via a thin catheter compared with sham treatment.3 Others have also pointed out that there is insufficient evidence that LISA is preferable to surfactant administration after intubation.4 It may also be a concern that a failed trial of LISA and the subsequent need of endotracheal intubation may cause prolonged hypoxia which is known to be associated with ICH.5
The Norwegian Neonatal Network (NNN) collects detailed information on infants admitted to all the neonatal intensive care units (NICUs) in Norway, including data on early surfactant administration and whether this is given by LISA or after endotracheal intubation. For extremely preterm (EPT) infants (GA<28 weeks), we aimed to investigate (1) to what extent LISA was used in Norway and (2) whether LISA was associated with benefits in terms of risk of death and cerebral and intestinal morbidities, need of and duration of MV, and prevalence of BPD. We hypothesised that these outcomes based on a large national quality register with diversity in intensive care practises might differ from outcomes obtained in trials conducted under standardised and more optimal conditions.
Material and methods
Participants
We included all live-born infants with GA less than 28 weeks admitted to the 16 Norwegian NICUs during 2012–2018 and registered in the NNN. With few exceptions, GA was based on routine ultrasound assessments at 17–19 gestational weeks, otherwise on the date of the last menstrual period. In Norway, treatment of infants with GA less than 26–28 weeks is centralised to seven university hospitals (hospitals 1–7, table 1). The other hospitals treated some infants with a GA above 26 weeks and some with a lower GA if the mother could not be transferred to a university hospital.
Infants born before 28 weeks’ gestational age (GA) during 2012–2018 in Norway
Data
The NNN systematically collected data on GA, birth weight (BW), sex, provision of antenatal steroids, mode of delivery, Apgar scores at 1 and 5 min, data allowing calculation of clinical risk index for babies II (CRIB II),6 survival during the initial hospital stay or age at death, treatment and mode of delivery of surfactant, days on MV, days on positive pressure respiratory support or supplemental oxygen to maintain oxygen saturation above approximately 90% as measured by pulse oximetry, occurrence of severe cerebral morbidity, defined as ICH grade 3 or 4 according to Papile et al7 or cystic periventricular leukomalacia (ICH/PVL), and verified necrotising enterocolitis (NEC), defined as Bell stage 2–3.8 We defined BPD as the need of supplemental oxygen or positive pressure respiratory support at postmenstrual age (PMA) 36 weeks (BPD-36).9 We also retrieved the same information at PMA 40 weeks (BPD-40) as a surrogate measure of severity of BPD. Small for gestational age (SGA) was defined as a BW below the 10th percentile for GA and sex according to Norwegian references.10
Exposure and controls
We defined LISA infants as infants who received the first dose of surfactant by thin catheter placed in the trachea. There was no national policy on indications or details on how LISA was performed. We compared LISA with two control groups: the rest of the cohort (non-LISA) and the non-LISA infants who received the first dose of surfactant after endotracheal intubation (non-LISA+S).
Statistics
Descriptive data are reported as means, medians, SD, 95% CIs, Spearman’s correlation, counts or proportions, as appropriate.
Because LISA was only used in 13/318 (4.1%) of infants with GA less than 25 weeks, we restricted comparisons to those with GA 25–27 weeks. First, we assessed if there were correlations between the rates of LISA and rates and mean duration of MV between NICUs. Correlations disclosed differences in background data and treatment policies between NICUs. We therefore used propensity score (PS) analyses to reduce potential bias when estimating the effect of administering LISA. First, we created a probability model for receiving LISA based on baseline variables thought to predict the use of LISA and/or the outcome variables: sex, GA, antenatal steroids or not, mode of delivery (vaginal vs caesarean section), Apgar score at 5 min, CRIB II score, year of birth and hospital of treatment. Most of these variables are also presented as central background data in the OPTIMIST trial.3 We used a mixed-effects logistic regression model, and, for maximum flexibility, GA, Apgar and CRIB II scores, and year of birth were modelled as non-linear terms—restricted cubic splines with three knots. Hospital was included as a random intercept. We used the estimated probabilities from this model (with conditional mode used for hospital effects) as PSs. For each LISA infant, we selected the non-LISA and the non-LISA+S infant with the closest PS within a calliper of 0.2 on the logit scale as a match (1:1 ratio), without replacement and with ties broken at random. With this method, we estimate the average treatment effect in those treated (ATT) with LISA, that is, the effect of receiving LISA among the subjects who received it. To assess the comparability of baseline characteristics, we report means or percentages of all variables included in the PS model both before and after matching.
We analysed the outcome variables from the PS dataset as non-paired, using Welch’s t-test to compare the number of days on MV for infants receiving LISA versus non-LISA and non-LISA+S. To estimate the expected difference in the number of days on MV at the individual (not population) level, remove the effect of any residual baseline imbalance and potentially increase the precision of the estimates, we additionally used a linear mixed-effects model with the same explanatory variables as in the PS model. We used χ2 tests to compare all categorical variables.
We performed two post-hoc sensitivity analyses, both for the PS and regression analyses: one after removing an infant with an unusually large number of days on MV, and one after removing CRIB II scores as a predictor variable, since the CRIB II score was missing for 40 infants. There were no other missing data in the predictors. One infant had missing data on NEC and was excluded from analyses involving this variable.
We used R V.4.1.211 for all analyses. The mixed-effect model was fitted by using the lme4 package V.1.1–V.27.1,12 and the PS matching was performed by using the ‘Matching’ package V.4.9–V.11.13 All CIs reported are 95% CIs.14
Results
Of 1174 registered infants (45% girls), 843 were born at GA 25–27 weeks and included in the analyses; 26% received LISA (figure 1). The use of LISA increased during the 7-year period, especially during the last 2 years (data not shown). There were marked differences in the use of LISA between hospitals (table 1). There was a positive association between hospitals regarding the proportion of infants who received LISA and the mean duration of MV (table 1, figure 2, Spearman’s r=0.75, p=0.001), but no convincing association between the proportion who received LISA and the proportion treated with MV (Spearman’s r=0.11, p=0.75).
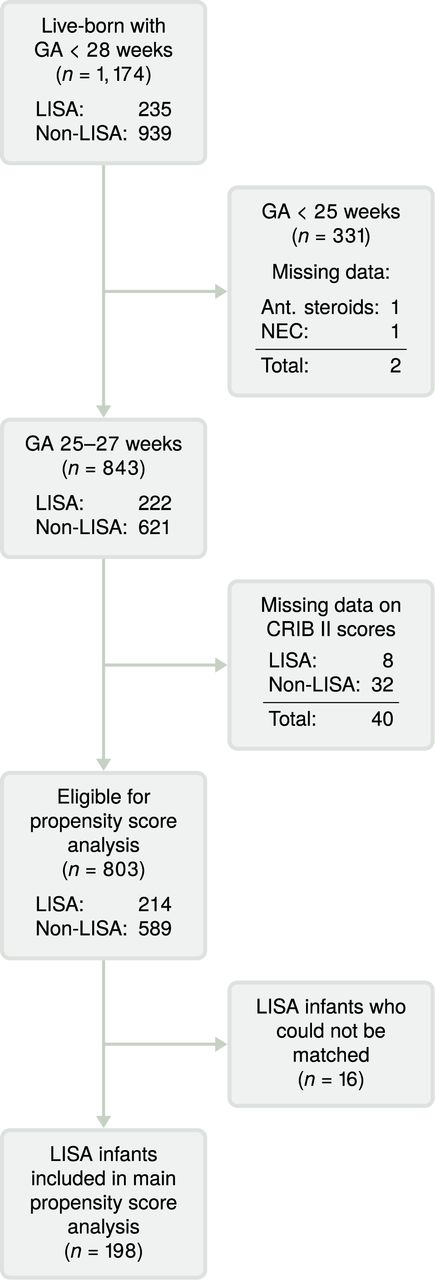
Patient flow chart for main analysis (n=1174). ant., antenatal; CRIB II, clinical risk index for babies II; GA, gestational age; LISA, less invasive surfactant administration; n, number of infants; NEC, necrotising enterocolitis.

Association between the proportion of infants with gestational age 25–27 weeks (n=843 infants, 16 hospitals) who received less invasive surfactant administration (LISA) in each hospital* and the proportion who received mechanical ventilation (MV) at that hospital (Spearman’s r=0.11, p=0.75), and the mean number of days** on MV (Spearman’s r=0.75, p=0.001). The size of each point is proportional to the number of infants born at the hospital. *The six smallest hospitals, with a total of ten infants, are grouped together and represented as one point. **Also including patients with no days on MV.
In unadjusted analyses, the LISA infants had higher survival rates at 7 days and at PMA 36 and 40 weeks, and lower rates of BPD-36 (42% vs 50%, p=0.03), but not of BPD-40 (12% vs 16%, p=0.17) than the non-LISA infants (table 2 and panel 1 in table 3). In contrast to the pattern when the data were aggregated to hospital level (figure 2), fewer LISA infants received MV (62% vs 81%, p<0.001), and the LISA infants had fewer mean days on MV than the non-LISA infants (8.3 vs 11.3 days, p=0.007, tables 2 and 3). There was no significant difference in days on MV between LISA and non-LISA infants who were ventilated (13 vs 14 days, p=0.69), nor on the proportion of the survivors who had ICH/PVL (8% vs 10%, p=0.34) or NEC (5% vs 5%, p=0.79) (table 2).
Infant characteristics according to gestational age at birth and stratified according to application of less invasive surfactant administration (LISA) versus a strategy of providing surfactant if needed after primary endotracheal intubation (n=1173)
Comparisons of outcomes for infants treated with less invasive surfactant administration (LISA) and the rest of the infants (non-LISA) before (panel 1) and after (panel 2) propensity score matching, and for LISA infants and infants who received their initial dose of surfactant after endotracheal intubation (non-LISA+S, panel 3) after propensity score matching
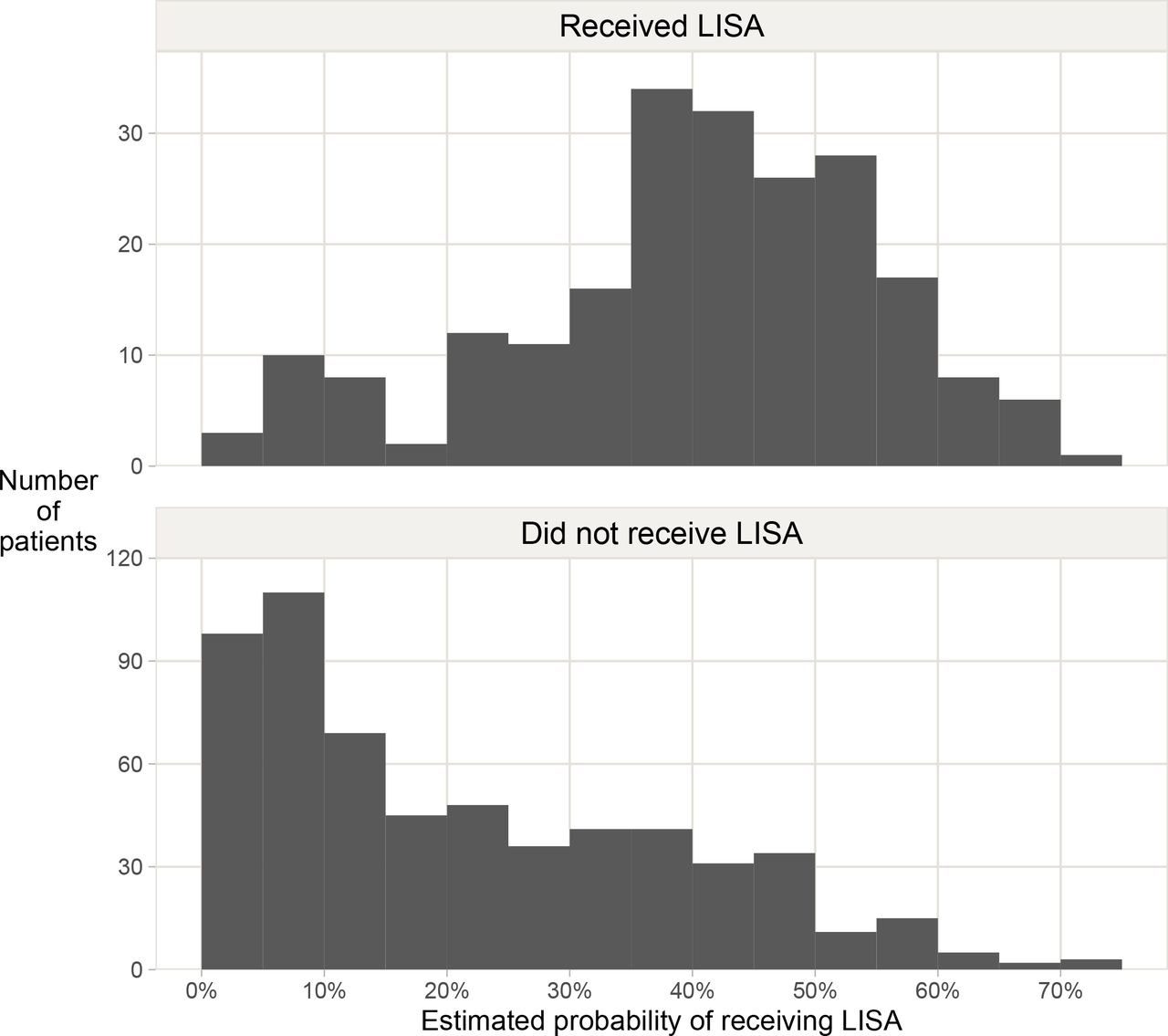
There was a suitable overlap in the PS distribution between the LISA and non-LISA infants (figure 3), and a match was found for 198 of the 214 LISA patients (93% matching success rate; eight LISA infants were excluded due to missing CRIB II scores). Before matching, there were differences in the distribution of baseline characteristics, most notably for Apgar score, but the LISA and non-LISA infants were similar across all major variables (table 4).

{kind=link}
{kind=link}
{kind=link}
Distribution of propensity scores stratified by use of LISA (n=803). The figure shows an overlap in the score distributions between the two groups of infants, which makes a propensity score analysis feasible. LISA, less invasive surfactant administration.
Balance of baseline characteristics for infants with gestational age 25–27 weeks (n=843) before and after propensity score matching for infants treated with less invasive surfactant administration (LISA) and the rest of the infants (non-LISA, panel 1), and for LISA infants and infants who received their initial dose of surfactant after endotracheal intubation (non-LISA+S, panel 2)
After PS matching, the survival rate was still marginally in favour of LISA compared with all non-LISA infants (table 3, panel 2), and the LISA infants had an estimated 4.1 (95% CI 0.0 to 8.2) fewer mean days on MV, also after adjusting for additional variables (4.1, 95% CI 0.3 to 8.0). After removing a non-LISA infant with 288 days on MV, the estimated mean difference was 2.7 days (95% CI −0.3 to 5.8, p=0.08). The difference in medians was 1 day in favour of LISA. There were minor differences between the LISA and non-LISA infants in the point estimates for rates of BPD-36 or BPD-40, NEC and ICH/PVL.
When restricting the analysis to the infants who received surfactant (LISA vs non-LISA+S, table 3, panel 3), a match was found for fewer LISA infants (146) in the PS analysis (table 4). In this subset, there was no longer any significant difference in survival, but days on MV was still in favour of LISA (mean difference 5.8, 95% CI 0.6 to 10.9 days, p=0.03). After removing the infant with 288 days on MV, the difference was 3.9 days (95% CI 0.3 to 7.5, p=0.03). For all analyses, the results were similar when CRIB II was removed from the PS model (results not shown).
Discussion
In this national multi-centre quality register study which included all EPT infants admitted to NICUs in Norway during 2012–2018, LISA was rarely used in infants born with a GA less than 25 weeks, but in around 1 of 4 infants born between GA 25 and 27 weeks. The rates of endotracheal intubation and MV varied substantially between NICUs but were unrelated to their LISA strategy. After PS matching, there were differences in favour of the LISA infants regarding rates and duration of MV, but no statistically significant differences in rates of neurological or gastrointestinal morbidities, or in rates and probably not in severity of BPD, since the decline in rates of BPD from PMA 36 to 40 weeks was the same for the LISA and non-LISA infants.
The positive association between NICUs regarding proportions treated with LISA and mean duration of MV probably reflects differences in both indications for treatment with surfactant and MV, and in accepting permissive hypercapnia before discontinuing MV. However, the PS analyses suggest that different treatment policies did not affect outcomes in terms of rates of BPD, or neurological or gastrointestinal morbidity. The lack of effect on occurrence of BPD corresponds with the result of the OPTIMIST trial, although the latter study had a different design.3 We speculate that the marginal effects of LISA in the PS models may be overestimated since the reason for electing LISA was not defined in the dataset; it is possible that infants who were intubated before surfactant administration in the NICUs with a LISA strategy had apnoea or more severe lung disease than those who received LISA.
The current European guidelines1 suggest early nasal CPAP as the first-line strategy in spontaneously breathing preterm infants with respiratory distress, and non-invasive surfactant administration, such as LISA, if respiratory distress is diagnosed. However, only two of the studies that these guidelines were based on included infants with GA 23–28 weeks15 16; most of the analyses also included or were restricted to more mature infants.15–30 To extrapolate recommendations based on the treatment of relatively mature and robust infants to more vulnerable infants carries a risk of causing harm, for example, from prolonged early hypoxia in the case when LISA fails to cause improvement. We found no evidence of increased harm associated with the use of LISA, and, reassuringly, no trend towards increased IVH/PVL. However, the study was not powered to conclude on these adverse outcomes. In the OPTIMIST trial, the mortality was higher in the LISA than in the control group for the infants born at GA 25–26 weeks, which may be a cause for some concern.3
The strengths of the study were the inclusion of virtually all liveborn EPT infants in Norway where resuscitation was attempted, and prospective collection of data in a uniform manner in a national quality register. In Norway, prenatal and postnatal life support is generally provided from GA 24 weeks, while decisions are made more individually at earlier GAs. The overlap in PS distribution, the resulting high (93%) matching success rate and the close balance in baseline characteristics after matching indicate that the PS model was suitable in reducing bias from confounders. There are, however, several limitations, including unavailable or unmeasurable confounders. For instance, BPD is a multifactorial disease, and unrecognised differences in care may have contributed to differences in a diagnosis of BPD-36 and BPD-40.31 32 Moreover, the study was underpowered to detect small differences in BPD incidence. It is also important to bear in mind that the PS analyses estimate the treatment effect for the patients actually treated with LISA (the ‘ATT’). The findings thus cannot be generalised to patients where LISA was not seen as a viable treatment option.
Conclusion
Our results suggest that the use of LISA may reduce the need for and duration of MV in infants born at GA 25–27 weeks, but that it has little or no effect on reducing mortality or pulmonary, neurological or gastrointestinal morbidity. Marked variations in the use of LISA and outcomes between NICUs may indicate that individual NICU routines may be equally or more important than a LISA versus a non-LISA strategy. Further research should aim at defining clinical circumstances where LISA may be clearly beneficial or potentially cause harm.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Relevant data are included in text. Data files may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Regional Committees for Medical and Health Research Ethics in Norway (Regional Comittee for Medical Research Ethics Western Norway, REK West) (Reference number 2015/2332, ID 29093). The Norwegian Neonatal Network collects personally identifiable data without consent according to the regulation of The Medical Birth Registry of Norway and the Personal Health Data Filing Systems Act of Norway.
Acknowledgments
We thank the neonatal units from the following hospital in Norway for contributing with data to the Norwegian Neonatal Network and thus making this study possible: Oslo University Hospital—Rikshospitalet, Oslo; Oslo University Hospital—Ullevål, Oslo; Akershus University Hospital, Lørenskog; Drammen Hospital, Drammen; Østfold Hospital Trust, Fredrikstad; Innlandet Hospital Trust, Lillehammer; Innlandet Hospital Trust, Elverum; Telemark Health Trust, Skien; Hospital of Southern Norway, Kristiansand; Hospital of Southern Norway, Arendal; Stavanger University Hospital, Stavanger; Haukeland University Hospital, Bergen; Fonna Health Trust, Haugesund; Sunnmøre Health Trust, Ålesund; Førde Health Trust, Førde; St. Olav University Hospital, Trondheim; Nord-Trøndelag Health Trust, Levanger; Nordland Central Hospital, Bodø; University Hospital of North Norway, Tromsø and Finnmark Health Trust, Hammerfest.
References
Footnotes
Contributors HR developed the concept and initiated the study, contributed to the analyses, interpretation and discussion of the results, made the first draft and had the main responsibility for completing the manuscript. HR accepts full responsibility for the work, had access to the data, and controlled the decision to publish. KOH was a biostatistician. He participated in developing the concept and had the main responsibility for the statistical analyses and construction of tables and figures. He participated in interpretation and discussion of the results and in writing the manuscript. He accepted the final version of the manuscript. AER has the main responsibility for the national neonatal registry. He participated in the provision of data, discussion on statistics, interpretation and discussion of results, and in writing the manuscript. He accepted the final version of the manuscript. CK participated in the discussion on statistics, in interpretation and discussion of the results, and in writing the manuscript. He accepted the final version of the manuscript. HJS has the main responsibility for the national neonatal registry. He participated in the provision of data, in the discussion on statistics and in interpretation and discussion of results, and in writing the manuscript. He accepted the final version of the manuscript. TM developed the concept together with Dr Reigstad. He contributed in the discussion on statistics, and in interpretation and discussion of the results and in writing the manuscript. He accepted the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.