Article Text

Abstract
Helicobacter pylori infection affects more than half of the world population and it occurs generally in childhood. It is associated with gastroduodenal ulcer, gastric atrophy, intestinal metaplasia, gastric adenocarcinoma and lymphoid tissue-associated lymphoma. It is difficult to eradicate this bacterium due to its high antimicrobial resistance. In children, the infection is asymptomatic in the majority of cases and complications are less common. Probable inverse relationships with allergic diseases and inflammatory bowel diseases are being studied. These reasons mean that the decision to diagnose and treat the infection in children is only considered in specific circumstances in which it provides true benefits. This review focuses on some current considerations regarding epidemiology, diagnosis and treatment of childhood infection, emphasising outcomes and treatment schemes in children.
- gastroenterology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Helicobacter pylori is a Gram-negative microaerophilic bacteria. It has been found in mummies, but was first described when it was related to chronic gastritis and peptic ulcer disease in 1983 by Barry Marshall and Robin Warren.1 This discovery was the beginning of numerous investigations to amplify knowledge of this bacterium.
The prevalence of infection in paediatric age is high and varies from country to country and in the same geographical area. It colonises the gastric mucosa generally in childhood, and passes asymptomatically in most patients, in which it will remain in the gastric cavity throughout life in the absence of eradication therapy.2 Infected patients may develop chronic active gastritis, peptic ulcer disease 10%, gastric cancer 1%–3% and will present with mucosa-associated lymphoid tissue lymphoma 0.1%. All these complications occur in their vast majority in adulthood.3 4 The development of the disease is related to the virulence of the strain, the genetic predisposition, the host’s immune response, the time of exposure and environmental factors. The CagA+ and VacA s1m1 strains are considered the most pathogenic and carry a higher risk of precancerous lesions. The risk seems higher if infection with these strains occurs simultaneously and in childhood.5 6
The prevalence of infection in adults tends to decrease in some parts of the world. The increasing resistance to antibiotics, as well as the lack of therapeutic alternatives that achieve 90% eradication effectively make infection a complex scenario.
The diagnosis and treatment should not be considered in the same way in children and adults. The immune mechanisms against infection differ at both stages of life and therefore the decision to investigate and treat infection in childhood is indicated in a small proportion of patients in whom the benefits are greater considering that recurrence and complications largely occur from ineffective treatments.
Epidemiology
H. pylori has infected approximately 50% of the total population.7 The prevalence is known in children worldwide and varies among countries. It is lower in high-income countries (34.7 %) than in low-income and middle-income countries (50.8 %), more prevalent in adults than in children and may also vary in a geographic area within a country.7 The highest rates have been cited in Nigeria, Serbia, South Africa, Nicaragua and Colombia with 89.7 %, 88.3 %, 86.8 %, 83.3% and 83.1%, respectively, and the lowest in Yemen, Indonesia, Belgium, Ghana and Sweden with 8.9 %, 10.0 %, 11 %, 14.2% and 15 %,8 respectively. In Latin America, 52% of children and adolescents are infected.9 Improvement in sanitary conditions, as well as decreased transmission have been the reasons why the prevalence has decreased in many parts of the world.
Transmission
Several studies describe that person-to-person transmission among family members is frequent, with mother-to-child being the most predominant and the most important transmission route being oral-oral and oral-faecal.10 Contaminated water can also be a source of infection, in which the bacterium can remain for long periods in a viable state. Many associate H. pylori infection with socioeconomic conditions and dietary habits, suggesting that foods such as milk, meat and vegetables may be an important route of transmission. Saliva is also another possible source of infection.11
Clinical manifestations
The infection is acquired around 10 years of age and approximately 85% have long asymptomatic periods.2 4 Clinical manifestations (table 1) are non-specific and some may be justified by the presence of complications. A statistically significant positive association with nausea, but no significant association between gastrointestinal symptoms, pain or pain characteristics and infection has been documented.12 Other studies have found that symptoms decrease in frequency and intensity or disappear with or without eradicating the bacteria. A meta‐analysis attempted to establish a possible association between infection and symptoms, and concluded that it was not related to vomiting, diarrhoea, flatulence, chronic functional abdominal pain, halitosis, regurgitation, constipation or nausea. However, they documented a statistically significant association with epigastric pain.13 Persistent vomiting, digestive bleeding, iron deficiency anaemia (IDA) of unspecified cause, malnutrition may be due to complications from the infection or another diagnosis and therefore require investigation.
Clinical presentation
H. pylori may a play role in some extraintestinal disease like unexplained IDA, immune thrombocytopenic purpura (ITP), Henoch-Schonlein purpura, bronchial asthma, other allergic diseases and inflammatory bowel disease (IBD). There are conflicting study results regarding the protection or inverse relationship of H. pylori and bronchial asthma, other allergic diseases and IBD.14 15 A meta‐analysis suggests that H. pylori may have immunoregulatory properties in IBD, and the inverse association seems stronger in paediatric patients and those with Crohn’s disease.16 17 Another meta-analysis supports the inverse relationship of infection with the risk of bronchial asthma, especially in CagA+ patient.18 Future research is required in this regard.
Diagnostic methods
There are multiple invasive and non-invasive methods for the diagnosis of H. pylori infection, with different levels of sensitivity and specificity (table 2).19 20 The initial diagnosis in children should be performed through invasive methods and the evaluation of the response through non-invasive methods.2
Diagnostic methods for Helicobacter pylori infection
The initial point of investigation in children begins with upper endoscopy or oesophago-gastro-duodenoscopy (OEGD) for different indications. Although this procedure does not allow direct diagnosis, with high-definition endoscopic techniques like Blue Light Imaging and Linked Colour Imaging are helpful in characterisation of mucosal changes in chronic gastritis, allowing the selection of areas for sample collection.21 The most frequent endoscopic diagnosis in children is nodular gastritis. Initially H. pylori colonises the antrum and can produce antral gastritis and if the infection persists nodular, pangastritis.10 This can also be observed in Crohn’s disease, cooeliac disease, allergic diseases, eosinophilic gastritis, collagen, autoimmune, lymphoma, cytomegalovirus infection and other infectious causes and therefore these causes must be ruled out. In this context, the infection can be diagnosed and the first challenge begins, in deciding whether to treat or not. OEGD should be indicated to investigate the cause of symptoms, not the presence of H. pylori infection.2
Unlike adults, gastroduodenal ulcers in children are infrequent. Samples should be taken for biopsy and the infection confirmed. Other causes, however, need to be considered. Gastric atrophy and intestinal metaplasia are less frequent as compared with adults,2 22 and are more related to time exposure.
During the procedure and for the initial diagnosis, at least six samples must be taken. Two samples, of the antrum and the body taken for histopathological study, for which the Sydney classification should be used. Two samples for culture, one from the antrum and the other from the corpus and lastly a sample for rapid urea test (RUT) or other molecular method: PCR or fluorescence in situ hybridisation (FISH).2
The sensitivity of all invasive methods is compromised by the use of antibiotics, bismuth, proton pump inhibitors (PPI) and upper gastrointestinal bleeding.
Culture has a specificity of 100% but the sensitivity is compromised by the use of antibiotics, H2-receptor antagonists, PPI, bismuth, alcohol drinking, digestive bleeding, high activity of gastritis, low bacterial load the quality of the sample collection, the patchy distribution of H. pylori, transport of biopsies, staff skills and culture media. For these reasons, it should not be used as the only diagnostic method. A negative culture does not exclude infection. This has the advantage of providing antimicrobial sensitivity data to offer strain-directed treatment. Ideal is to provide this method for initial diagnosis but when it is available generally is reserved for cases with a first time failure.2 19 20
However, it is known that in vitro sensitivity does not always respond to successful eradication in vivo, patients may be colonised by several strains, also strains isolated in various sites may have different susceptibilities to antimicrobials, additionally a patient may have multi-resistant strains.
PCR provides excellent specificity and sensitivity. It also allows detection of specific mutations leading to antibiotic resistance, such as fluoroquinolone and macrolides. It is more reliable to detect hetero-resistant status. PCR can also be performed from stool samples, saliva and gastric juice. Studies reported a more frequent CagA+ VacA s1m1 in children and adolescents.4 19 20
RUT is a very cheap and fast method, with a good sensitivity and specificity, although the sensitivity is affected in young children, with the use of antibiotics, PPI, bismuth and digestive bleeding.
Histology allows for the presence of bacteria to be identified. Provides details of the activity, degree of chronic inflammation, presence of lymphoid follicles, diagnosis of coccoid forms and also premalignant lesions such as atrophic gastritis and intestinal metaplasia that lead to close monitoring of the patient. To improve the sensitivity, it is important to take several samples. Neutrophil infiltration is less significant in children than adults but infiltration by lymphocytes, plasma cells and immunosuppressive T regulatory cells are more significant.2 19 20
Non-invasive methods are not indicated to make an initial diagnosis of infection in children. The stool antigen test (SAT) and 13C-urea breath test (UBT) are used to evaluate eradication and are indicated 4 weeks after the end of treatment. These tests are only used as initial research when investigating causes of ITP, only if EGD cannot be performed.2 If the SAT is positive after treatment, it is prudent to perform UBT in children. Some studies recommend that, after the eradication confirmed by these methods, an annual non-invasive technique should be performed, especially in areas of high prevalence or in at-risk individuals, for the recrudescence diagnosis.2 11
Antibody-based tests for H. pylori in serum, whole blood, urine and saliva are not modified by treatment with PPI or antimicrobials but their utility is more accurate for epidemiological purposes. The antibodies remain for a time after eradication and it does not allow differentiate between current and past infection.
Diagnosis
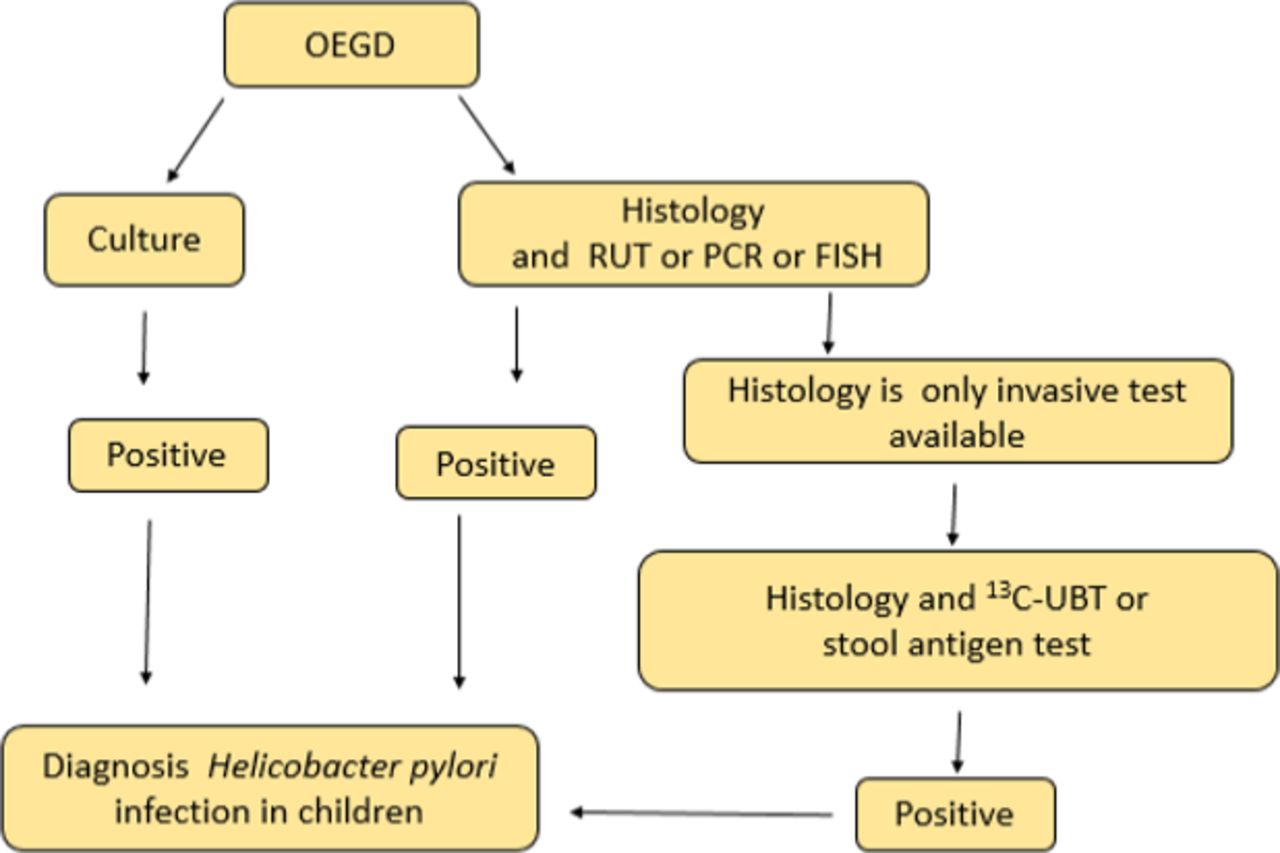
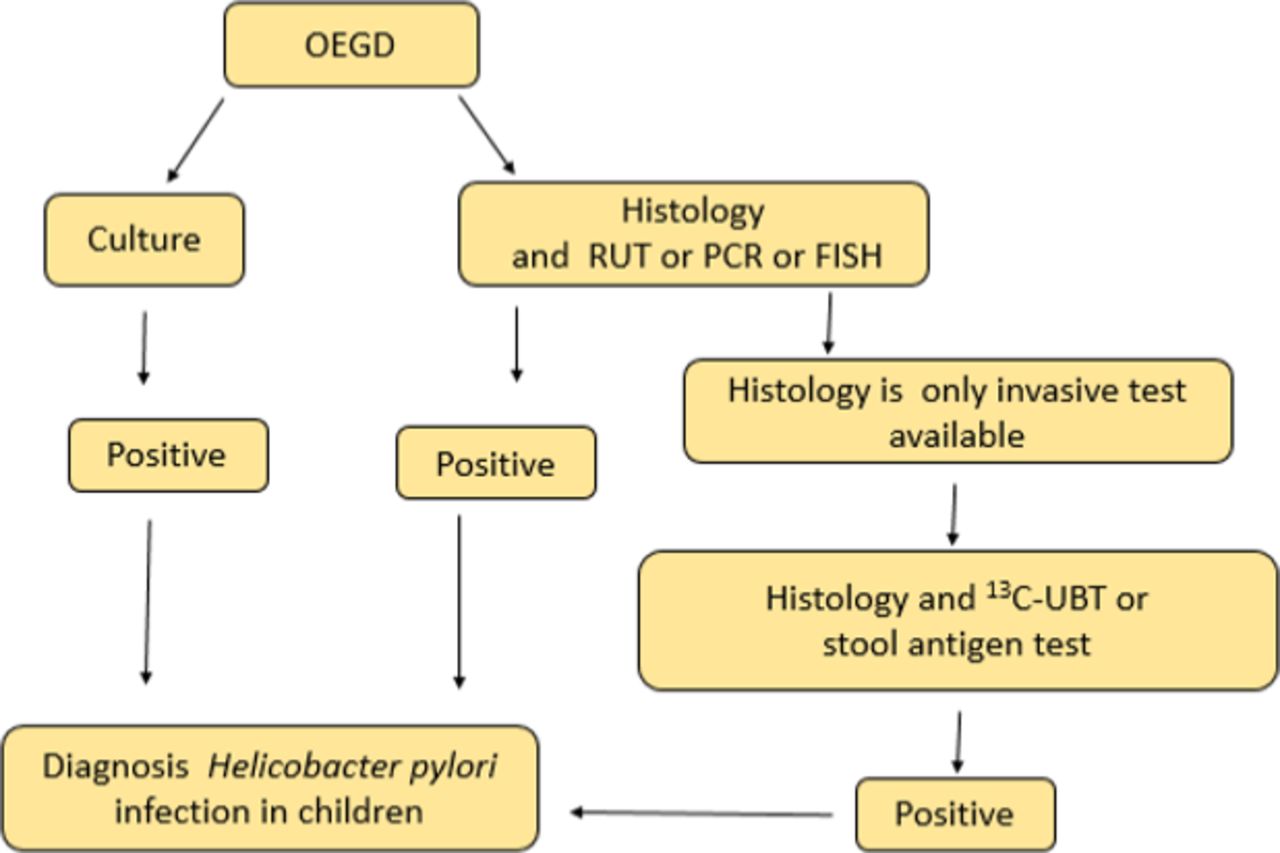
In children the diagnosis is confirmed through invasive methods and is limited to patients in whom benefits are expected: in gastroduodenal ulcer and/or erosive gastritis, refractory IDA in which other causes have been ruled out and when investigating causes ITP.2 The diagnosis is confirmed by the following (figure 1):
{kind=link}
Legends13C-UBT: urea breath test; OEGD: oesophago-gastro-duodenoscopy; FISH: fluorescence in situ hybridisation; RUT: rapid urea test.
Positive culture.
If culture is not available or is negative: two invasive methods (histology and RUT or some molecular method: PCR or FISH).
If culture is not available or it is negative and only histology is available, a non-invasive method can be used (UBT or SAT).
Treatment
Without a treatment scheme, eradication is highly improbable. Spontaneous eradication is described mainly in infants and young children; the eradication decreases with age.23 Research and treatment in children is controversial due to the prevalence of infection in a geographical area, the incidence of age-related cancer, high rates of antimicrobial resistance along with the presence of complications associated with H. pylori. It would be beneficial to treat at an age that reinfections are less probable (>12 years) before reaching non-return premalignant lesions, such as atrophic gastritis and intestinal metaplasia.24 The most virulent strains increase the risk of cancer three times, all can cause chronic inflammation and diseases; hence, it is not necessary to know the strain to decide to treat.25
Treatment is indicated in children with gastroduodenal ulcer and refractory IDA in which other causes have been ruled out. Eradication of H. pylori infection need to be also considered in patients with ITP.26 In contrast, for asymptomatic children, chronic functional abdominal pain, short stature, first-degree family with gastric cancer and family with H. pylori infection, treatment is not indicated.2 In those patients in which the diagnosis is incidental histopathological finding during OEGD performed for other possible diseases, IBD, eosinophilia disease, among others, only should be treated after an analysis with the parents or legal relatives in which they should be oriented in favour of treatment (risk of complications at later ages) and against (infrequency of complications at this age, reinfections, adverse reactions, change in the intestinal microbiota, possible protective effects against other diseases, reduces the alternatives for subsequent treatments if necessary and the need for treatment adherence to achieve successful eradication).2
Treatment regimens for first-line therapy should provide a cure rate of at least 90%. Excessive indication of antibiotics or ineffective treatment regimens for H. pylori infection has led to an increase in the resistance of key antibiotics for treatment.
Adapting the first line of treatment according to susceptibility would be ideal (table 3), but we know that in practice it is difficult so therefore in many regions treatment is indicated empirically. Clarithromycin (CLA) is the choice of treatment in patients with susceptible strains. If the resistance rate exceeds 15%–20% in that region, it should not be used unless sensitivity to this antibiotic is known in the patient2 4; therefore, in patients with known sensitivity to CLA and metronidazole (MET), the first recommended option is PPI-AMO-CLA. They can use sequential therapy as alternative treatment. In those with known resistance to CLA, triple therapy with PPI-AMO-MET is indicated, and PPI-AMO-CLA for those with resistance to MET. In both cases, bismuth therapy can be used as an alternative treatment. Patients with unknown susceptibility or double resistance are not recommended to treat with PPI-AMO-CLA. Triple therapy with high doses of AMO can be considered as the first line of treatment, as well as bismuth-based and concomitant therapy as treatment alternatives. Treatment regimens and doses are based on European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and North American Society for Paediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) guidelines.2
First-line therapy
There is high resistance to CLA and MET, mainly CLA in children and MET in adults. It varies with region and is an increasing trend.4 In the studies reviewed in children within the last 5 years, we observed that in most of them the resistance rates to CLA and MET exceed 20%, with CLA resistance prevailing and with very little resistance to amoxicillin (AMO) and levofloxacin.27–29 Multidrug resistance was a problem.27 28 30 Resistance increases considerably in treatment failures.28 31 The hetero-resistance in strains was described in children.27 Studies demonstrated that triple therapy with PPI-AMO-CLA offers acceptable eradication rates when the strains are sensitive, and the resistance to MET does not significantly influence eradication.32–34 Authors reported patients with susceptibility-guided treatment with adherence >90% of treatment achieved acceptable rates of eradication,30 35 the rates were significantly higher in those receiving sequential therapy.35 High doses of MET with triple therapy for 10 days in patients without culture improved eradication rates, although the desired ones were not achieved.34 One study (although with limitations) compared four schemes in patients who had not received previous treatments. Therapies with bismuth, concurrent, sequential and triple therapy were offered for 14 days; eradication rates of 89.8 %, 84.6 %, 74.1% and 69.5% were achieved. There was no significant difference between the adverse effects in the regimens used, despite prolonging the duration of sequential therapy; it was not possible to improve the eradication rate.36
PPI plays a key role in treatment; double doses are recommended to improve susceptibility to AMO and CLA and to overcome rapid degradation with individual differences of CYP450 cytochrome polymorphisms. Vonoprazan is a potent antisecretory that is used in children, achieving rates higher than those obtained with PPI-AMO-CLA for a period of 7 days eradication.37 The bismuth is a drug that has been shown to have effect against H. pylori. Studies in adults have shown that it improves the efficacy of the antimicrobials used and has offered better results in patients with resistance to CLA.38 MET resistance can be partially overcome if doses are increased and treatment days are prolonged. Levofloxacin or tetracycline may be used in children older than 8 years.2
After a failure in the first therapy, it would be necessary to determine antimicrobial resistance before the next treatment.2 Treatment schemes in rescue therapies can be seen in table 4.
Rescue therapies
A meta-analysis on the use of probiotics in H. pylori infection suggested that supplementation with Lactobacillus to treatment improves adverse effects such as diarrhoea when used at higher and longer doses. It may benefit eradication.39
Recurrence of infection can occur by recrudescence or reinfection. Recrudescence is when a strain that caused the recurrence is genetically identical to that isolated before receiving the eradication treatment, and reinfection is when the strain is genetically different. Recurrence rates are reported during the 3–12 months after eradication, decreases over time, declining sharply after 1 year.23 Annual reinfection rates are lower than those of recrudescence and are extremely low in high-income countries. Reinfection in children over the age of 5 and adults is considerably low. After eradication, the maintenance of documented negativity for 1 year or more may be an indicator against recrudescence. Therefore, an ineffective therapy appears to produce a recrudescence of infection.11 40
Studies between different treatment regimens in children are mostly based on comparing sequential therapy and triple therapy in 10–14 days with standard PPI doses. In those treatments in which the susceptibility is unknown, acceptable rates were nor achieved. Sequential therapy shows no benefits by extending it to 14 days. For treatment selection, it is necessary to know the local rates of antimicrobial resistance and if they are not available, at least to know which is locally reliable, it is necessary to know the drug history with macrolides, nitroimidazoles and quinolones.
Treatment should be individualised according to susceptibility for 14 days (except sequential therapy) with high doses. The use of probiotics can be beneficial since it improves the adverse effects of the medication and therefore the adherence to the treatment that is necessary for a successful eradication. Further studies related to adherence of different treatment regimens, higher doses of PPI and quadruple therapies, especially in patients with unknown susceptibility, multiresistant strains and treatment failure are needed. In adults, many studies suggest quadruple therapies as the first line of treatment.
Conclusions
The decision to investigate and treat H. pylori infection in children should be based on providing true benefits, taking into account the low frequency of complications at this stage, the recurrence of infection, the probable inverse relationships with allergic and immunological diseases, antimicrobial resistance as well as the few treatment alternatives available for treating the infection in children.
Acknowledgments
The authors thanks Dr. Adrian Van-Nooten for his linguistic advice
References
Footnotes
Contributors The following document includes the participation of each author in the manuscript. Everything was recorded on the basis of the joint decision. IA-M: planned the study, searched and selecting articles in the PubMed and Cochrane Library search engines, performed analysis and interpretation of data, writing of the manuscript, approval of final version and responsible for overall content. SED-O: searched and selecting articles in the PubMed and Cochrane Library search engines, performed analysis and interpretation of data, writing of the manuscript and approval of final version. AAE: searched and selecting articles in the PubMed and Cochrane Library search engines, approval of final version and manuscript review. OMVJ: searched and selecting articles in the PubMed and Cochrane Library search engines, writing of the manuscript and approval of final version. YdCVV: writing of the manuscript and approval of final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study. There are no data in this work.