Article Text

Abstract
Background In Ethiopia, 38% of children less than 5 years of age are stunted and 57% are anaemic. Both have a negative impact later in life on physical growth and cognitive development and often coexist. There are few studies in Ethiopia that assessed co-morbid anaemia and stunting (CAS) and context-specific factors associated with it.
Objective The objective of this study was to assess the prevalence of CAS, and factors associated with CAS among children aged 2 to 5 years, in southern Ethiopia.
Methods A community-based cross-sectional survey was conducted among 331 randomly selected children in 2017. Mothers were interviewed using a structured questionnaire to obtain child and household information. Anthropometric measurements and blood samples for haemoglobin were collected. Stunting was defined as height-for-age Z-scores (HAZ) less than −2 SDs and anaemia was defined as altitude-adjusted haemoglobin levels less than 11.0 g/dL. CAS was defined when a child was both stunted and anaemic. Crude and adjusted multinomial logistic regression analyses were used to identify factors associated with CAS.
Results Out of 331 children studied, 17.8% (95% CI 13.87% to 22.4%) had CAS. Factors found significantly linked with higher odds of CAS were increased child age (adjusted OR (AOR) 1.0 (1.0 to 1.1)) and no iron supplementation during the last pregnancy (AOR (95% CI) 2.9 (1.3 to 6.2)). One factor found significantly linked to lower odds of CAS was food secured households (AOR (95% CI) 0.3 (0.1 to 0.9)).
Conclusions Co-morbid anaemia and stunting among children in the study area is of concern; it is associated with household food security, iron supplementation during pregnancy and child age. Therefore, comprehensive interventions focusing on improving household food security and promoting iron supplementation for pregnant women are suggested.
- epidemiology
- syndrome
- growth
Data availability statement
Data are available on reasonable request. Also, data can be available on reasonable request from the corresponding author AZO (zalemselam@yahoo.com; ORCID: https://orcid.org/0000-0001-8300-2412?lang=enhttps://orcid.org/0000-0001-8300-2412?lang=en).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
One in four children 6–24 months of age had anaemia and stunting in Ethiopia based on the Ethiopian Demographic and Health Survey.
Vitamin A supplementation, consumption of vitamin A–rich fruit and vegetables, meat and legumes, meal frequency, low household wealth, low caregivers’ education level, male sex, age, history of infection and small birth size have been found associated with anaemia and stunting in children less than 2 years of age in Ethiopia.
What this study adds?
One in six children 2–5 years of age in southern Ethiopia had co-morbid anaemia and stunting.
Food insecurity, child age and iron supplementation during pregnancy were associated with co-morbid anaemia and stunting among children 2–5 years of age.
Background
Globally, 22% of children less than 5 years old were stunted in 20171 and about 42% were anaemic.2 According to the Ethiopian Demographic and Health Survey (EDHS) of 2016, 38% of children less than 5 years of age were stunted and 57% were anaemic.3 When looking only at the age group of 2–5 years, the recent study in Ethiopia reported 33% of prevalence for anaemia4 and 45% of prevalence for stunting.5
Both anaemia and stunting during early life can lead to serious health effects later in life such as increased susceptibility to infections and chronic diseases, impaired cognitive and physical development, and low economic productivity of individuals and the society.6–8 Chronic anaemia has a negative effect on physical growth during all stages of growth (infancy, childhood and adolescence).9
Both anaemia and stunting share common risk factors such as poverty, poor sanitation, large family size, low nutrient intake and infections.10 11 In recent years, there has been a growing interest to conceptualise and address syndemic health problems including malnutrition.12 13 In public health nutrition, a syndemic health problem is defined as the aggregation of two or more nutritional health problems in a population with factors that exacerbate the burden of disease.12 A systematic review of demographic and health survey (DHS) data from 46 low-and-middle-income countries showed that the prevalence of co-morbid anaemia and stunting vary by country and socioeconomic groups.14 The same study suggests that co-morbid anaemia and stunting should be considered under a syndemic framework, the Childhood Anaemia and Stunting (CHAS). The syndemic approach aggregates anaemia and stunting, and also acknowledges social and environmental factors that exacerbate the occurrence of stunting and anaemia. This approach can be more useful in resource-constrained settings as the prevention strategies focusing on stunting and anaemia differs.14
The Ethiopian government is working to reduce child malnutrition by promoting dietary diversity, deworming, iron supplementation during pregnancy, malaria prevention and nutrition education.15 16 Despite several interventions, both anaemia and stunting remain the largest nutritional problems among children.3 17 There are several studies in Ethiopia which have investigated the prevalence and determinant factors of either stunting or anaemia.18–21 However, studies on co-morbid anaemia and stunting are few. The only study reporting national data to our knowledge was based on an analysis of EDHS data that reported 24% prevalence of co-morbid anaemia and stunting in children younger than 2 years.11 Furthermore, a controversial idea was that a study from Asia reported that anaemia and stunting are independent conditions22 opposing a systematic review from low-and-middle-income countries recommending that stunting and anaemia should be considered as a syndemic.14 Therefore, more research is needed on context-specific findings in terms of co-morbidity and risk factors. This study aimed to assess the prevalence of co-morbid anaemia and stunting and associated factors among children 2–5 years old in southern Ethiopia. Thus, the findings could inform planning of nutrition interventions to mitigate the problems.
Methods and materials
Study area and population
We conducted a cross-sectional study among children aged 2–5 years from 15 February to 30 March 2017 in Cheffe Cote Jebessa kebele (lowest administrative unit in Ethiopia), located in the semi-urban part of Hawassa City, in southern Ethiopia. Hawassa City is located in South Nation, Nationality and People Regional State, 273 km from Addis Ababa, the capital of Ethiopia. According to a census, we conducted before the start of our study, the total population of the village (Kebele) was 23 010 people within 3900 households, and 2180 children were less than 5 years of age. The main crops cultivated in the study area include maize, haricot beans, inset and Irish potatoes. Based on our observation during census and survey, the study area (Kebele) is characterised by poor economic status, inadequate health facilities, poor environmental hygiene and sanitation, and inadequate water supplies.23
Sample size and sampling procedure
The sample size was calculated using anaemia prevalence because this study was a part of a larger study that aimed to evaluate the efficacy of home-processed amaranth grain containing bread in the treatment of anaemia among 2-to-5-year-old children in southern Ethiopia.24 Thus, the sample size of 340 was calculated assuming a 33% national average anaemia prevalence among children aged 3–5 years,17 95% confidence level and ±5% margin of error. A post hoc sample size calculation done for this study was 281 assuming a 24% CAS prevalence, 95% confidence level and ±5% margin of error.11 From the list of 1689 children aged 2 to 5 years residing in the study area, 340 were selected by a simple random technique method using IBM SPSS V.20. Participants were eligible if the child was 2 to 5 years of age and residing with their mother who provided informed consent. We selected the age group 2–5 years old for our experimental study, as children would be fed with the prepared bread. We excluded children who were sick or suffering from severe medical conditions.
Study variables
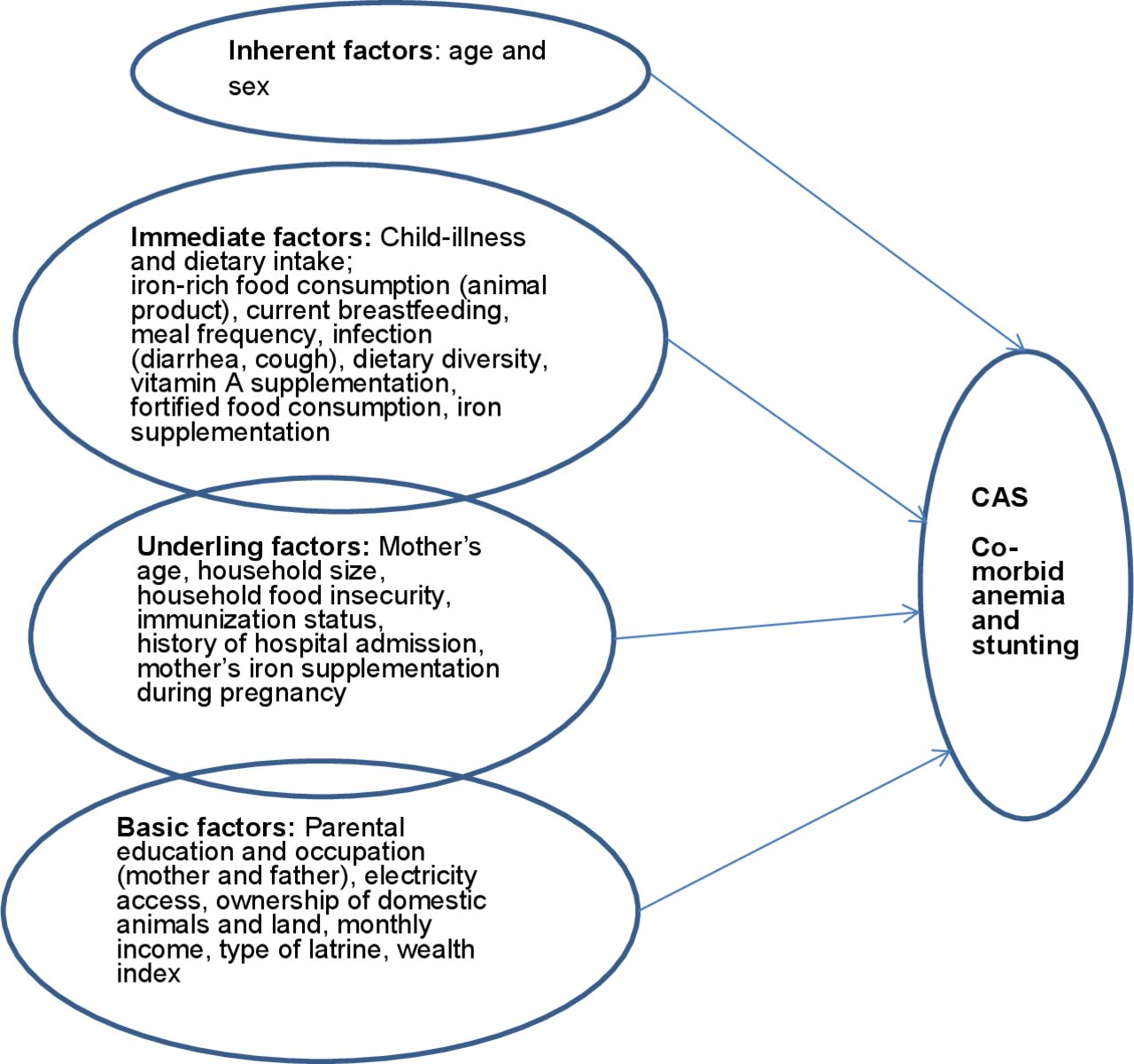
The primary outcome variable of this study was co-morbid anaemia and stunting (CAS), defined when a child was both anaemic and stunted. Secondary outcomes were anyone having either stunting or anaemia. Stunting was defined as height for age (HAZ) z-scores below −2 SD whereas anaemia was defined as altitude adjusted haemoglobin values <11 g/dL.25 Independent variables were selected based on the conceptual framework from Unicef where the variables were grouped into inherent, immediate, underlying and basic factors.26 The specific factors in each group are given in the illustration (figure 1).
{kind=link}
Conceptual framework used in the multivariable regression analysis based on the Unicef framework from 1991.26 The model is sorting the variables as inherent, immediate, underlying and basic risk factors for co-morbid anaemia and stunting, CAS.
Data collection
Data were collected from mothers on various demographic, socioeconomic, health and nutrition variables using a structured questionnaire. Seven-day food frequency (FFQ) and 24-hour dietary diversity questionnaires were used to collect information about children’s diets. The questionnaires were adapted to the study area based on Food and Agriculture Organization guidelines.27
Household food insecurity status was measured by using the Household Food Insecurity Access Scale (HFIAS) developed by the Food and Nutrition Technical Assistant (FANTA) project and validated in Ethiopia by Ghebreyesus et al.28 The HFIAS is composed of nine items, which are asked with a recall period of 1 month. For each item, there was a follow-up of the frequency of the occurrence question. If they experienced the item, they were asked whether they experienced it rarely (once or twice in the past month), sometimes (three to ten times in the past month) or often (more than ten times in the past month). Responses were scored so that ‘never’ received a score of 0, ‘rarely’ scored 1, ‘sometimes’ scored 2 and ‘often’ scored 3, so that when summed, the lowest possible score was 0 and the highest 27. The household’s food security status was categorised into four levels of food security according to the categorisation scheme recommended by the HFIAS Indicator Guide.29
Anthropometry and haemoglobin measurements
Height was measured using a Seca 213 portable stadiometer (Seca 213; Seca GmbH, Hamburg, Germany), and the height of the child was read to the nearest 0.1 cm. Weight was taken using a calibrated digital Seca874 scale (Seca 874, Seca GmbH) electronic flat scale. Emergency Nutrition Assessment for SMART software 2011 (Toronto, Canada) was used for analysis of anthropometric data. Weight and height measurements were converted to height-for-age (HAZ), weight-for-age (WAZ) and weight-for-height (WHZ) z-scores, based on WHO reference standards. For HAZ, z-scores <−2 indicated stunting and >−2 indicated normal height.30
Using vein puncture, 3–5 mL of blood was collected by using a lithium heparin plasma separator test tube to measure haemoglobin. The blood was shaken slowly six to eight times prior to measuring haemoglobin levels, which were determined immediately on-site using a HemoCue analyser 301 (Angelholm, Sweden). The HemoCue analysers were calibrated every morning before the start of data collection. Then haemoglobin was corrected for altitudes, according to WHO standards.31 Anaemia was defined as altitude-adjusted haemoglobin values<11.0 g/dL.25
Socioeconomic status
Principal component analysis was used to assess household wealth index. The presence or absence of each household items such as access to electricity, ownership of a radio, telephone, television, refrigerator, electric stove, bicycle, motorcycle, car or computer were asked and their responses were coded as ‘0’ for No and ‘1’ for Yes. The first component explained 32% variance and sampling adequacy test was 0.77. Finally, the common factor score for each household was produced for grouping households as poor, medium and richest wealth thirtiles.
Statistical analysis
Data were double-entered and checked using EpiData V.3.1 (EpiData.dk, Odense, Denmark), independent variables were selected for multivariable model using R Core Team V.4.1.0 (2021) and analysis was done using IBM SPSS V.20. Descriptive statistics (frequency counts and percentages) were used to summarise categorical variables. Continuous variables were presented using means and 95% CIs, median with IQRs and prevalence estimates were reported along with CIs.
Before doing multinomial analysis, the dependent variable was assumed nominal and mutually exclusive. The dependent variable consists four nominal categories: ‘no anaemia or stunting’, ‘stunting only’, ‘anaemia only’ and ‘stunting and anaemia together’ (CAS). The ‘no anaemia or stunting’ category was set as the reference. Complete case analysis was used for missing values to minimise potential bias. Twenty-three potential factors associated with CAS were identified based on a conceptual framework (figure 1), and then 10 variables were selected according to minimum lambda using least absolute shrinkage and selection operator (LASSO) for multinomial logit model; this was implemented using glmnet package of R (online supplemental table 1). Thus, the 10 selected independent variables were analysed with multinomial logistic regression model to identify factors associated to CAS.
Supplemental material
Results
Child characteristics
From a total of 340 children selected for the study, 331 (97.4%) participated in the study and 9 (2.6%) of the mothers refused to provide the written consent as the survey involved blood sample collection from their children. Of the 331 children involved in the study, 172 (52%) were girls and the mean age was 39.3 (95% CI 38.0 to 40.5) months. Close to three-fourths of the children, 242 (73%), had the lowest dietary diversity score. About 15 (4.5%) of children consumed fortified food and only 10 (3%) children received iron supplementation (table 1).
Characteristics of the study children aged 2–5 years in Cheffe Cote Jebessa kebele, southern Ethiopia, 2017
Socioeconomic characteristics of the study households
The median age of mothers was 27 years (IQR 24–30). The majority of the mothers, 231 (69.8%), were housewives. More than half, 169 (51%), of the household size was greater than five people per household. Three-quarters of the households had a monthly income which was less than 1900 Birr per month (which is <US$1.90 per day) and 207 (62.5%) households were food insecure (table 2).
Socioeconomic characteristics of the study household in Cheffe Cote Jebessa kebele, southern Ethiopia, 2017
Magnitude of CAS)
More than half of the children, 173/331 (52.3%), had either anaemia or stunting. The prevalence of stunting was 125/331 (38%) (95% CI 32.5% to 43.1%), and for anaemia it was 107/331 (32%) (95% CI 27.3% to 37.4%). The overall prevalence of CAS among the study participants was 59/331 (17.8%) (95% CI 13.7% to 21.9%) (table 3).
Magnitude of stunting, anaemia, and co-morbid anaemia and stunting
Factors associated with CAS)
Crude ORs compared for factors were considered in the study and the outcomes are presented in online supplemental table 2. The adjusted multinomial logistic regression showed that child age, iron supplementation during pregnancy and household food security status were associated with CAS.
Supplemental material
From the inherent factors, when child age increased by 1 month, it increased the likelihood of the occurrence of CAS (adjusted OR (AOR) 1.0 (1.0 to 1.1)). From the underlying factors, children from a mother who did not take iron supplementation during the last pregnancy were three times more likely to develop CAS (AOR 2.9 (1.3 to 6.2)) compared with those who took iron supplementation during last pregnancy. Further, CAS was less common in children who lived in food secure households (AOR 0.3 (0.1 to 0.9)) as compared with children who lived in food insecure households (table 4).
Factors associated with CAS, anaemia and stunting among the study participants in Cheffe Cote Jebessa kebele, southern Ethiopia, 2017
Discussion
This study described that almost one-fifth of children were affected by CAS. It was associated with child age, father’s educational status, iron supplementation during pregnancy and household food security status.
The 18% prevalence of CAS was lower than the study done in Ethiopia among younger children 6 to 23 months of age that reported a 24% prevalence of concurrent anaemia and stunting.11 This variation may be due to the different age groups and the use of national demographic health data. In the DHS data analysis from different low-income countries, the national prevalences of co-morbid stunting and anaemia among children aged 6–59 months were 25% in Ethiopia, 22% in Gabon and 25% in Congo.14
Stunting, with 38% prevalence, is categorised as a severe nutritional public health problem in the study area. Our finding is comparable with the study done in Ethiopia reporting 41% of stunting among children under 5 years of age.32 Furthermore, an anaemia prevalence of 32% is categorised as a moderate public health problem of children aged 2–5 years in the study area. This finding is similar to a study from northern Ethiopia finding a prevalence of 37% in children less than 5 years of age.19
We found that children living in food secured household had lower odds of CAS than those in food insecure households. A higher anaemia prevalence20 and stunting prevalence33 in food insecure households have been reported previously in Ethiopia. Food insecure households could have limited access to diversified food and had lower meal frequency than food secure households. The study done in Ethiopia among children showed that low meal frequency significantly increases the co-occurrence of stunting and anaemia.11 In our study, meal frequency was not associated with CAS but food insecurity may have had a relationship with meal frequency. Similarly, studies conducted in Ethiopia showed that stunting was high among children who had low meal frequency, less than four times per day, compared with those who had more frequent meals.34 35 The explanation could be that children who get frequent meals, whatever its content would be, probably get more nutrients. This is supported by the study undertaken in Ethiopia which reported inadequate energy intake and low-quality protein consumption as the main cause of stunting.36 Low meal frequency and low energy intake could be aggravated by household food insecurity.
In this study, we found that children born to mothers who took iron supplements during their last pregnancy were less likely to develop CAS than those who had mothers who did not get supplements during pregnancy. We have not found other studies that have investigated the relationship between iron supplementation during pregnancy and CAS in children. However, some studies report on low iron intake of mothers and having a mother with symptoms of anaemia as predictors for anaemia in children less than 5 years of age.10 37
In this study, increased child age had higher odds of CAS than those in the lowed age. However, we could not find similar studies supporting these findings related with CAS, but there are studies which showed similar results for stunting.38 This may be due to growth impairment becoming more severe with time. Anaemia has shown various associations with age as multiple issues including the mother’s nutritional status, breast feeding and diet, genetic issues and co-morbidity may be closely related to it.10
Strength and limitation
Our study is one of few studies done in Ethiopia presenting CAS and contextually relevant co-factors. The study used a representative sample using a simple random sampling technique at a community level. However, the study area was selected purposively since this study was a part of a larger study that aimed to evaluate the efficacy of home-processed amaranth grain containing bread in the treatment of anaemia among 2-to-5-year-old children in southern Ethiopia.24 Also, our sample size calculation based on the EDHS 2011 report since our proposal development and approval was before the release of the 2016 EDHS report. Furthermore, children aged 3–5 years were used for sample size calculation as EDHS was not reporting on the age group 2–5 years. Moreover, we used validated questionnaires, and standard and calibrated haemoglobin, height and weight measurements. As this study used a cross-sectional design, caution should be exercised in evaluating cause–effect relationships.
Conclusion
In conclusion, our study provided a concerning high-level co-morbid anaemia and stunting among children in the study area, which was associated with household food security status, child age and mother’s iron supplementation during pregnancy. The high prevalence of anaemia and stunting at the same time indicates that it is necessary to tackle both burdens simultaneously. Policy-makers should promote and strengthen the implementation of the iron supplementation during pregnancy as a short-term implementation strategy and improving household food security as a long-term implementation strategy to treat children with CAS.
Data availability statement
Data are available on reasonable request. Also, data can be available on reasonable request from the corresponding author AZO (zalemselam@yahoo.com; ORCID: https://orcid.org/0000-0001-8300-2412?lang=enhttps://orcid.org/0000-0001-8300-2412?lang=en).
Ethics statements
Ethics approval
The institution ethical board of Hawassa University (IRB/098/08) and the Regional Ethical Committee West of Norway (No. 2016/2034) provided ethical approval. Local administrative and health post authorities granted official permissions to undertake the study. Informed written consent was obtained from mothers for the study participants.
Acknowledgments
The authors are grateful to Mr. Damte Data Daba, field coordinators, all data collectors, Cheffe Cote Jebessa Health Centre, all health post workers, Cheffe Cote Jebessa community leaders and all study participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ingunnengebret1
Correction notice This article has been corrected since it was first published. A new affiliation for the co-author 'Eskindir Loha' has been added.
Contributors AZO conceived the research idea, implemented the study, collected the data, performed the statistical analyses and drafted the manuscript. EL, BL and IMSE participated in developing the research idea, proposal review, data analysis and critical review of the draft manuscript. IMSE also participated in the training of the data collectors and the evaluation of the pre-test. All authors approved the final version of the manuscript.
Funding The funding body of this research was NORHED/SENUPH (Norwegian Program for Capacity Development in Higher Education and Research for Development/South Ethiopia Network of Universities in Public Health).
Disclaimer The role of the funding body was covering the administrative cost of the research but had no role in the design of the study and collection, analysis, and interpretation of the data, and writing the manuscript.
Authors declared that there is no computing interest. Authors declared that there is no computing interest.
Patient and public involvement statement Patients or the public were not involved in the design, conduct, reporting and dissemination plans of our research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.