Article Text

Abstract
Background Monitoring of peripheral capillary oxygen saturation (SpO2) during neonatal resuscitation is standard of care in high-resource settings, but seldom performed in low-resource settings. We aimed to measure SpO2 and heart rate during the first 10 min of life in neonates receiving positive pressure ventilation (PPV) according to the Helping Babies Breathe (HBB) protocol and compare results with SpO2 and heart rate targets set by the American Heart Association (AHA).
Methods A cross-sectional study was conducted at Mulago National Referral Hospital, Kampala, Uganda, as a substudy of the NeoSupra Trial. SpO2 and heart rate were measured on apnoeic neonates (≥34 weeks) who received PPV according to HBB (room air). Those who remained distressed after PPV received supplemental oxygen (O2). All resuscitations were video recorded and data were extracted by video review at 1 min intervals until 10 min post partum. Data were analysed for all observations and separately for only observations before and during PPV.
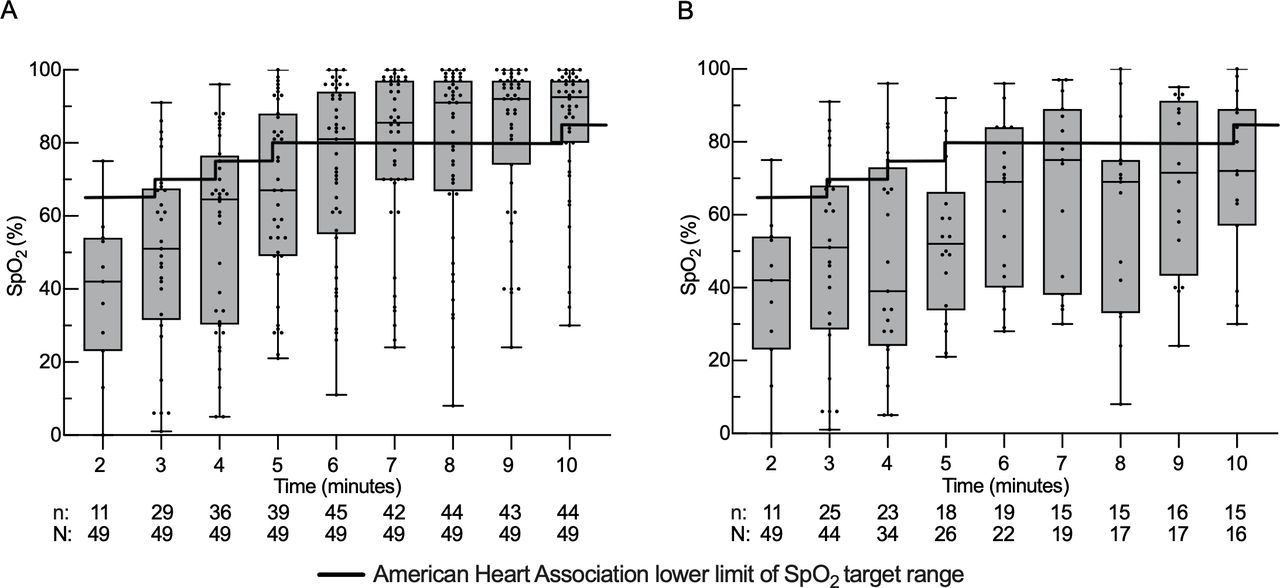
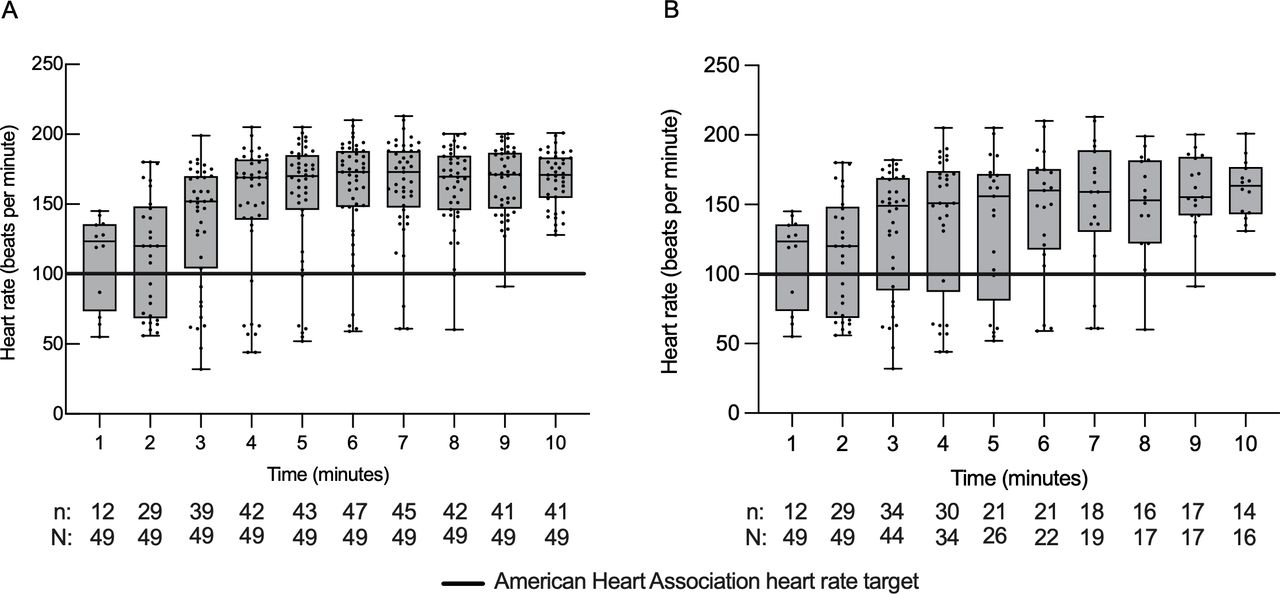
Results 49 neonates were analysed. Median SpO2 at 5 min (n=39) was 67% (49–88) with 59% of the observations below AHA target of 80%. At 10 min median SpO2 (n=44) was 93% (80–97) and 32% were below AHA target of 85%. When only observations before and during PPV were analysed, median SpO2 at 5 min (n=18) was 52% (34–66) and 83% were below AHA target. At 10 min (n=15), median SpO2 was 72% (57–89) and 67% were below AHA target. Median heart rates were above AHA target of 100 beats/min at all time intervals.
Conclusions A high proportion of neonates resuscitated with PPV after birth failed to reach the AHA SpO2 target in this small sample, implying an increased risk of hypoxic-ischaemic encephalopathy. Further studies in low-resource settings are needed to evaluate baseline data and the need for supplemental O2 and optimal SpO2 during PPV.
Trial registration number This is a substudy to the trial ‘Neonatal Resuscitation with Supraglottic Airway Trial (NeoSupra)’; ClinicalTrials.gov Registry (NCT03133572).
- neonatology
- resuscitation
- physiology
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. All original data for this substudy is available as a supplemental material. Background data can be made available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Oxygen saturation (SpO2) targets after birth for healthy neonates have been defined by the American Heart Association (AHA).
There have been few studies in low-resource countries measuring SpO2 in asphyxiated neonates.
What this study adds?
Measurement of SpO2 during neonatal resuscitation with video-based observation in a hospital setting in sub-Saharan Africa.
A high proportion of neonates resuscitated with positive pressure ventilation after birth failed to reach the AHA SpO2 targets in a Ugandan hospital.
Introduction
Each year, 7 million neonates need positive pressure ventilation (PPV) after birth.1 In 2015, 700 000 died of birth asphyxia, nearly half in sub-Saharan Africa.2
In term and late preterm neonates, PPV should be initiated using room air instead of 100% oxygen,1 3 4 since there is a significant reduction in short-term mortality.5 Pulse oximetry is recommended to guide oxygen therapy and maintain oxygen saturation (SpO2) within the normal ranges.3 4 6 This practice is supported by clinical consensus, but there is a paucity of studies assessing SpO2 during PPV in term infants.3 7 8 In low-resource settings, availability of blended oxygen and pulse oximetry is scarce and not included in guidelines aimed for this context,9 such as Helping Babies Breathe (HBB).10
Feasibility to reach SpO2 targets has been described among resuscitated neonates <32 weeks’ gestational age and found to be mostly outside of target ranges.11 12 For neonates >32 weeks, the feasibility of reaching targets is unknown.8 In 2007, Saugstad et al published a report on SpO2 in asphyxiated neonates receiving room air or 100% oxygen and described SpO2 levels in parity with current targets.13 14 A study from Kathmandu, comparing early versus late cord clamping in late preterm and term resuscitated neonates, reported SpO2 levels below American Heart Association (AHA) target range.15 To our knowledge, that is the only study assessing SpO2, conducted in a low-resource setting, using the HBB protocol, where no oxygen during PPV was provided.
This study aimed to investigate SpO2 and heart rate in the first 10 min after birth in neonates who received PPV according to the HBB protocol in a high-volume hospital in sub-Saharan Africa and compare results with SpO2 and heart rate targets set by the AHA.
Methods
Study design, setting and population
This cross-sectional observational study was conducted in January–July 2019 as a substudy of the NeoSupra Trial at the Mulago National Referral Hospital, Uganda, the largest public hospital in Kampala (altitude of 1200 m above sea level) with approximately 25 000 births each year.16 17 Most deliveries at this hospital present as emergencies, such as severe obstructed labour, fetal distress, antepartum haemorrhage or severe pre-eclampsia.
Resuscitations were performed by midwives trained in HBB and indication for PPV was apnoea or gasping. The attending research physician could intervene and supervise the resuscitation if needed, still following HBB. Oxygen was not provided during PPV according to the HBB protocol.18 After termination of PPV, neonates could receive oxygen by nasal cannula 0.5–5 L/min if showing breathing difficulties and cyanosis at midwifes’ discretion, according to hospital guidelines. Both neonates born through caesarean section (CS) in the operation theatre and by vaginal delivery in the labour ward were included by convenience when a research physician was available. Inclusion criteria were inborn neonates, estimated gestational age ≥34 weeks, estimated birth weight ≥2000 g, need for PPV at birth and parental consent. Exclusion criteria were any major malformation, incompatible with sustained life or affecting the airways, and stillbirth.
Study procedure
Immediately after birth, neonates eligible for inclusion had their cord cut and were taken to the resuscitation table where drying, stimulation, suctioning and PPV were initiated by a midwife. The research physician, who attended all births included in this substudy, placed a pulse oximeter probe (Philips reusable M1193A neonatal wrap sensor) on the neonate’s right hand as soon as possible and connected it to a pulse oximeter (Philips Intellivue X2, Amsterdam, The Netherlands). Heart rate was measured by dry-electrode ECG NeoBeat Newborn HR Meter (Laerdal, Stavanger, Norway),19 which was also placed as soon as possible after the neonate arrived on the resuscitation table. All cases were video-recorded using an HD1080P Black Box AI-IP018 camera (Shenzen Aishine Electronics Co, China). SpO2 and heart rate were measured during the first 10 min after birth. Time of birth, time from birth to table, amniotic fluid appearance, Apgar score, and mother and neonate clinical characteristics were collected and recorded by research assistants on-site.
Video recordings were reviewed by an investigating physician. SpO2, heart rate, and signal quality were visually observed on video and registered every minute for 10 min after birth. If data could not be acquired at the predetermined time interval because of a hidden display or unsatisfactory signal quality, the data point was collected at a time span of ±5 s from the determined time interval. If no data could be collected within this time span, it was registered as missing data. SpO2 signal was considered reliable if signal quality indicator showed medium-quality signal or better, if the plethysmograph curve showed continuous uniform waves of at least peak-to-peak amplitude of 50% between the top and bottom line or if heart rate on pulse oximeter and ECG were congruent within a range of 5 beats per minute (bpm). When heart rate by ECG was not available, heart rate measurements from pulse oximeter were used. The ECG signal quality was considered reliable if numbers were seen with sharp background on the display and unreliable if background was blurred. Observations from video review were manually entered into an Excel (Microsoft, Redmond, Washington, USA) spreadsheet.
Outcome
Outcome measures were SpO2 and heart rate in the first 10 min after birth, and the proportion of neonates with SpO2 below the AHA target at 5 and 10 min after birth.3 The outcome measures were assessed for all observations and separately in the subgroup of observations before and during PPV at each time point.
AHA states the following preductal SpO2 ranges after birth: 1 min 60%–65%, 2 min 65%–70%, 3 min 70%–75%, 4 min 75%–80%, 5 min 80%–85% and at 10 min 85%–95%,3 based on studies in healthy term neonates.6
Patient and public involvement
Neither patients nor the public were involved in design, or conduct, or reporting or dissemination plans of the study.
Data analysis
Since this was an explorative study, a priori sample size calculation was not performed but a sample of approximately 50 neonates was estimated sufficient to obtain representative data. Data analysis included video observations on SpO2 and heart rate with reliable signal quality available at each minute interval. Data were presented as numbers and proportions for categorical variables, means and SDs for normally distributed continuous variables, and medians and IQR for variables with skewed distribution. GraphPad-Prism V.9 (GraphPad Software, San Diego, California, USA) was used for statistical analysis and graphs. A subanalysis was made including only observations before and during PPV at each minute interval. Proportions of neonates with SpO2 below target ranges at 5 min and 10 min after birth were calculated for both groups. Heart rate of >100 bpm was considered as an indicator of adequate ventilation.3 4
Results
Neonatal characteristics
Sixty-eight neonates were initially selected for inclusion, of which 19 were later excluded. Reasons for exclusion were: one stillbirth; one declined verbal consent and three resuscitations that were not captured on video. Fourteen neonates were excluded since SpO2 data from the video recordings were unavailable due to late positioning of the pulse oximeter probe, difficulty to see oximeter display on video or unreliable SpO2 signal quality. The final dataset included 49 neonates.
Neonatal and maternal characteristics are reported in table 1, together with data from the face mask (FM) group of the main study, NeoSupra Trial.17 Apgar score at 5 min was <5 in 30% of neonates and <7 in 76%. Seventy-three per cent presented meconium-stained or foul-smelling amniotic fluid. Time to achieve first SpO2 measurement was 163 s (IQR 132–222) and PPV was started within the first minute in five neonates (10%). Supplemental oxygen was administered to 21 neonates after PPV (due to difficulty of breathing or cyanosis). Ten neonates (20%) died in the first week of life out of which six died after resuscitation in the delivery room (table 2).
Maternal and neonatal characteristics and data from the main study NeoSupra Trial*
Delivery room interventions, hospitalisation and clinical outcome
In the FM group of the NeoSupraTrial, 89% (n=530 of 597) of neonates were hospitalised and 11% (n=67 of 597) died after resuscitation; 18% (n=109 of 597) were found dead at 7-day follow-up.
As there were no reliable SpO2 observations in the first minute after birth, data referred to this time point were excluded from analysis (figure 1). Missing SpO2 data were more frequent at early time intervals and due to late attachment of the pulse oximeter probe and unreliable SpO2 signal quality (figure 1). Heart rate observations were also mostly missing the first minutes due to late positioning of pulse oximeter and ECG probes or bad signal quality (figure 2).
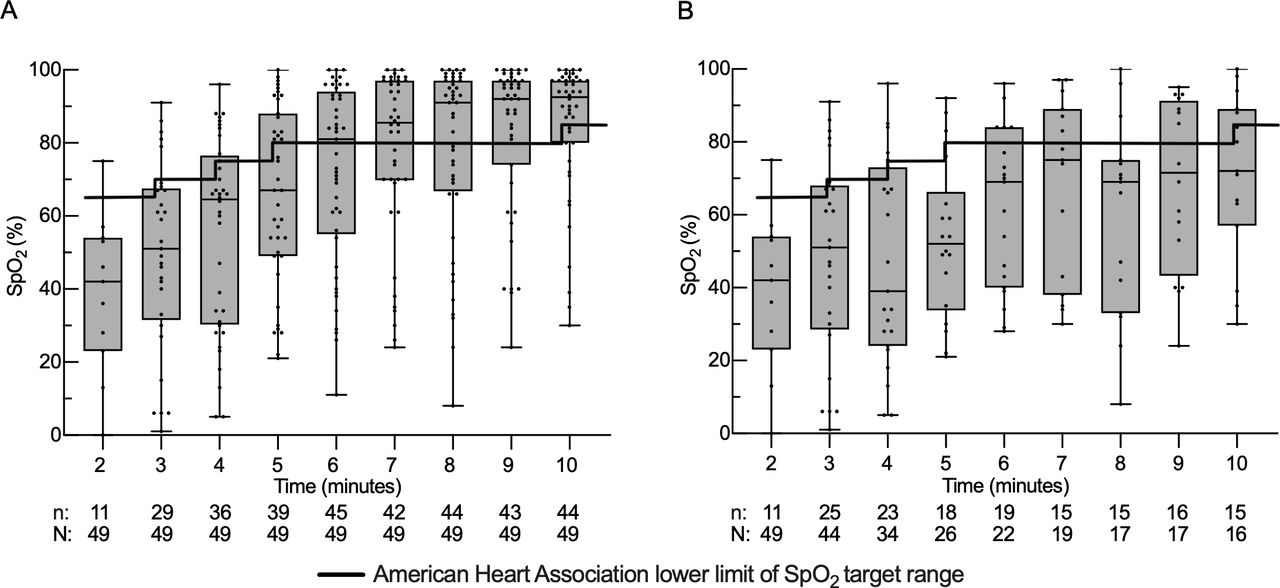
Preductal peripheral capillary oxygen saturation (SpO2) by pulse oximetry at 2–10 min after birth presented as box plots showing the median, quartiles, range (min and max values) and individual data points. Observations obtained (n) and sample size (N) are shown below the graph. (A) SpO2 observations of all neonates at each time point. (B) SpO2 observations of neonates before and during positive pressure ventilation at each time point.

{kind=link}
{kind=link}
Heart rate measured by dry-electrode ECG or pulse oximetry at 1–10 min after birth presented as box plots showing the median, quartiles, range (min and max values) and individual data points. Observations obtained (n) and sample size (N) are shown below the graph. (A) Heart rate observations of all neonates at each time point. (B) Heart rate observations of neonates before and during positive pressure ventilation at each time point.
All observations
SpO2 values from 2 to 10 min after birth are shown in figure 1A. When analysing all observations, median SpO2 level was below AHA target from 2 to 5 min after birth (figure 1A). At 5 min after birth, 59% of all neonates (n=39) had SpO2 values below the AHA target, and at 10 min (n=44) the proportion was 32% (table 3). Of the 21 neonates receiving oxygen supplementation because of difficulty of breathing after PPV, seven (33%) had SpO2 above AHA target range (85%–95%) at 10 min.
SpO2 values and proportion of neonates with SpO2 below American Heart Association (AHA) target
A post hoc analysis was made separating the 36 neonates with meconium-stained, foul-smelling amniotic fluid or both from those 13 neonates with clear amniotic fluid. In the meconium group, median SpO2 at 5 min was 79% (IQR 50–88, n=26) and 50% were below AHA target. At 10 min, median SpO2 was 94% (IQR 86–97, n=31) and 26% were below AHA target. In the group with clear amniotic fluid, median SpO2 at 5 min was 57% (IQR 46–68, n=12) and 75% were below AHA target. At 10 min, median SpO2 was 84% (IQR 59–95, n=12) and 50% were below AHA target.
Observations before and during PPV
When only observations before and during PPV were included in the analysis, the median SpO2 was below AHA target at all time intervals (figure 1B). The proportion of neonates with SpO2 below AHA target at 5 min after birth was 83% (n=18) and at 10 min 67% (n=15) (table 3).
Heart rate
Median heart rate was above target of 100 bpm at each minute interval for both all observations and only observations before and during PPV (figure 2A,B). At 2 min, 12 observations were below target in both groups and decreased every minute thereafter. At 10 min, no observations were below this target.
Discussion
In this observational study, a high proportion of resuscitated neonates had SpO2 values below AHA target in the first 10 min after birth, while heart rate remained above 100 bpm for the most part of the measurements.
The strengths of the present study include (1) data collection from review of video recordings allowing detailed monitoring of observed parameters, signal quality and hence enhanced reliability of data20 21; (2) the assessment of SpO2 and heart rate in a low-resource setting where PPV is performed in room air without the SpO2 monitoring.
Few studies have observed SpO2 during neonatal resuscitation. In a study by Saugstad et al, median SpO2 in neonates resuscitated with room air was 90% (5th–95th percentile 66–95, n=100) at 5 min and 90% (83–96, n=110) at 10 min, median Apgar score 4, 7 and 8 at 1, 5 and 10 min, respectively.13 Our corresponding figures were 67% (IQR 49–88) and 93% (80-97). Reasons for lower saturation at 5 min could be quality of resuscitation, observational method or severity of the asphyxia. Three-quarters of neonates in this study had Apgar score <7 at 5 min, associated with increased risk of mortality and morbidity.22–24 In Nepal, mean SpO2 levels in an early cord clamping group who received PPV (n=45) were 76.1% (SD 3.9) at 5 min and 85.1% (SD 2.8) at 10 min. SpO2 at 10 min was somewhat lower than in our study and results were also below the AHA targets.15 In both studies, SpO2 data were collected by direct observation and not by video review. SpO2 in neonates at high altitude (>4000 m above sea level) has been shown to be lower compared with measurements at sea level.25 Another study at similar altitude as Kampala observed comparable SpO2 at birth with the reference study at sea level by Dawson et al (median 69% vs 66% at 1 min), and we assume the altitude had a minor impact on our results.6 26
The high SpO2 dispersion reflects the variability of illness in resuscitated neonates. In our study, 43% of the neonates received oxygen after PPV (upon midwives’ assessment of breathing difficulties or cyanosis). This probably increased median SpO2, especially from 5 min after birth. Still, large proportions of patients (59% at 5 min, 32% at 10 min) had an SpO2 below AHA target. When only neonates before and during PPV were analysed, the proportion was even more prominent (83% at 5 min, 67% at 10 min) (table 3). Yet, most neonates had heart rate above 100 bpm, which is considered a sign of adequate ventilation (figure 2).3 4 This suggests that adequate PPV alone is not sufficient to achieve SpO2 in the recommended range. Though, since no respiratory function monitoring was used, conclusions about adequacy of PPV is not possible to make. This study observed a large portion of neonates with either meconium-stained, or foul-smelling amniotic fluid, or both indicating meconium aspiration. This could theoretically explain the low SpO2 in this sample, but a post hoc analysis surprisingly showed higher SpO2 in the group with meconium-stained amniotic fluid. A finding hard to interpret, but high rate of missing data in the meconium group and the small sample size are possible explanations. Persistent hypoxia in asphyxiated neonates may exacerbate pulmonary hypertension and have short-term and long-term consequences of hypoxic-ischaemic encephalopathy.27 Oxygen is not included in the HBB algorithm, since it is scarce and difficult to administer in blended form in low-income contexts,10 28 but the availability of oxygen in sub-Saharan African hospitals is increasing.29 30 A neonatal resuscitation algorithm for low-resource and middle-resource settings that includes oxygen has been proposed.31 The present study might support its use. Nevertheless, preventing dangerous hyperoxia is also recommended3 4 7; of note, 33% of neonates receiving supplemental oxygen after PPV had SpO2 levels above target range (>95%) at 10 min. These findings suggest that SpO2 measurement would be considered also in low-resource settings because the agreement between the assessment of infant colour and SpO2 is limited.32
The questions regarding supplemental oxygen still remain: oxygen or not, when and how much? Our results raise the question if these neonates would benefit from supplemental O2 during PPV. However, transferring a practice from one context to another may have detrimental effects.33 Caution must be taken not to implement an advanced resuscitation algorithm before the basic skills of good quality PPV have been mastered. Safe and accessible devices to blend and titrate oxygen need to be available as well as SpO2 monitoring to avoid both hypoxia and hyperoxia. Optimal saturation and oxygenation for neonates in need of PPV needs to be further investigated.7 8
This study has some limitations. It was an exploratory investigation with a limited number of participants which prevented calculations of CI and hence results can be difficult to generalise. Neonates were selected by convenience sampling based on the research physician’s availability, with risk for selection bias. However, baseline characteristics were in broad agreement with the NeoSupra Trial (table 1).17 Of note, the observed high rate of CS (84%) was partly due to convenience sampling but also due to lack of oximeter visibility on video recordings from the labour ward resuscitation table, where vaginal deliveries were performed. This was one of the main reasons for exclusion of neonates initially selected for analysis. Dawson et al reported that healthy babies born by CS are known to have lower SpO2 compared with those by vaginal delivery.6 It is difficult to assess if the high rate of CS affected the results in these severely asphyxiated neonates. This observational study suffered from missing SpO2 and heart rate data, particularly immediately after birth. This seems to be a random data loss that would not affect the results but implies an uncertainty to the data, especially at the initial time intervals. Median time to start of ventilation (123 s) in this study was markedly above the aimed for ‘golden minute’ (first minute of life), indicating difficulties in compliance with the HBB algorithm, mostly due to prolonged stimulation and suctioning. The delay in ventilation is a possible explanation of the low SpO2 in our study and it would be interesting to see if SpO2 improves with earlier start of ventilation. Time to PPV from birth in an earlier cohort at the same hospital was 137 s (n=99) and 92 s (n=48) after CS, indicating the problem is recurring.34 This is however not an issue unique to our study site. In a video observation study of 76 neonates from a hospital in Tanzania (where numerous HBB studies have been undertaken) that included rigorous HBB training, median time from birth to first ventilation was 108 s and the total duration of stimulation and suctioning before first ventilation was 45 s.35 A study from Mozambique found similar delays in ventilation after training.36 These examples highlight the difficulty in reaching the HBB target in this setting and we believe our results might reflect the situation in other busy hospitals in sub-Saharan Africa.
Conclusions
A high proportion of neonates resuscitated with PPV after birth failed to reach the AHA SpO2 target in this small sample, implying an increased risk for hypoxic-ischaemic encephalopathy. Further studies in low-resource settings are needed to evaluate baseline data and the need for supplemental O2 and optimal SpO2 during PPV with long-term follow-up on mortality and neurological outcome.8
Supplemental material
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. All original data for this substudy is available as a supplemental material. Background data can be made available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was part of the NeoSupra Trial,16 approved by the Institutional Review Board of Mulago National Referral Hospital, Uganda; the Uganda National Council of Science and Technology; the Director General from the Ministry of Health, Uganda (MREC 1168); and the Regional Committee for Medical and Health Research Ethics (REK South East reference number 2017/989) in Norway. A two-tier procedure for consent was used. All women admitted to the labour ward during the study period were given brief verbal information of the trial and provided oral consent. Written deferred consent was sought from mothers, whose neonates met inclusion criteria.
Acknowledgments
We would like to give our greatest appreciation to the staff at the Maternity and Neonatal Special Care Unit of Mulago National Referral Hospital, Kampala, Uganda, for their wonderful work to improve the care of neonates. We want to give special thanks to Francesco Cavallin (Independent Statistician, Solagna, Italy) for his invaluable comments on the manuscript. We also want to thank Josaphat Byamugisha and Jolly Nankunda (both Mulago National Referral Hospital) for their important contribution to the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @SavingNeonates
Contributors ML was responsible for the study design, data analysis, interpretation of data and contributed to preparation of the study site. He conducted the literature research and was responsible for the writing process of the manuscript and approval of the final draft. SMH contributed to study design and to the acquisition of data. She was responsible for preparation of the study site, revised the work draft, approved the final draft and act as guarantor of the study. AM was responsible for acquisition of data, contributed to preparation of the study site and approved the final draft. TT contributed to study design, revised the work draft and approved the final draft. CL contributed to study design, manuscript revision and approved the final draft. DT contributed to study design, interpretation of data, manuscript revision and approved the final draft. KE contributed to study design, data analysis and interpretation of data. She revised the work draft and approved the final draft. NJP contributed to study design, data analysis, interpretation of data and literature research. He was responsible for preparation of the study site, revised the work draft, approved the final draft and act as guarantor of the study.
Funding This was a substudy of the NeoSupra Trial supported by unrestricted grants from the Research Council of Norway (grant 250531) and the Centre for Intervention Science in Maternal and Child Health (project number 223269), Norway. Queen Silvia Children's Hospital, Paediatric Department contributed with a grant for the first author to work on the manuscript. In-kind contributions were made by the University of Bergen and Stavanger University Hospital, Norway; Makerere University, Uganda; Karolinska Institutet and Sachs’ Children and Youth Hospital, Sweden; and Padua University, Italy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.