Article Text

Abstract
Language barriers, if not adequately addressed, can prevent effective communication, impact patient safety and experience. Our research on language preference within the paediatric inpatient and outpatient services in west London revealed that 20% and 56%, respectively, would prefer to communicate in an alternative language than English. When we conducted emotional mapping analysis patients reported feeling ‘invisible’ and ‘not involved’ due to the lack of communication in their preferred language. Here, we describe our analysis and pilot intervention of using translated asthma care plans that aims to improve patient care, experience and outcomes by minimising the impact of language barriers.
- Health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Language barriers, if not adequately addressed, can prevent effective communication, impact patient safety and experience.1 Here, we describe a pilot project that aims to improve language services and provide a more inclusive service for our diverse paediatric population in west London.
Our aim was to improve paediatric services for patients who prefer to communicate in alternative language than English. Our objectives were to:
Determine the prevalence of patients’ who prefer to communicate in an alternative language.
Gain insights into patients’ experience.
Design a small-scale intervention to improve patients’ experience.
To understand language preference within the paediatric service we conducted the following studies in November 2021:
Prospective analysis of inpatients’ language preference.
Retrospective analysis of outpatient appointments’ language preference.
Emotional mapping—a form qualitative data collection—with three families receiving care.
The project was registered and reported to two groups within the Trust: ‘Population Health Steering group’ and ‘Asthma Big Room’ to ensure compliance with information governance and research standings.
The prospective analysis included 42 patients over the 5 consecutive days. Twenty per cent (n=9) stated their preference is to receive communication in an alternative language, with Arabic (n=6) being the most common alternative language. The majority of the admissions were due to respiratory-related illness.
Between November 2020 and October 2021, there were 44 039 outpatient attendances, where language preference was only recorded for 27% (n=12 083). For those with their language preference recorded (n=12 123), 44% preferred to communicate in English but 56% of attendees preferred to communicate in 39 different languages. Table 1 summarises the recorded five most common languages spoken in the outpatient context.
Children’s and young people outpatient appointments’ top five language preference (November 2020–October 2021)
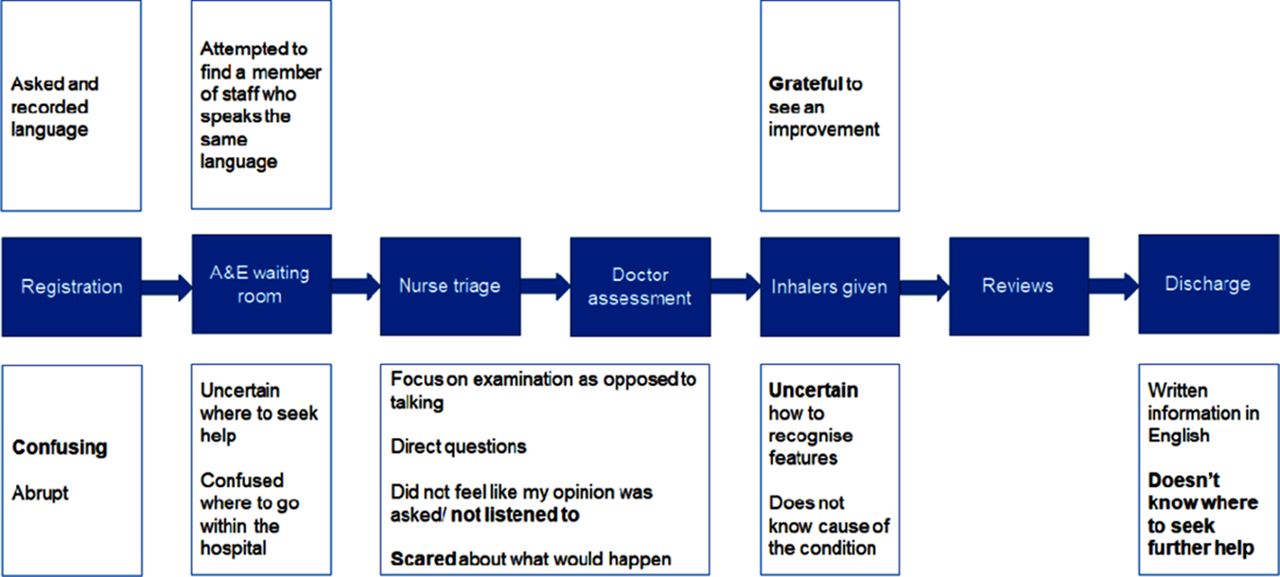
Emotional mapping analysis revealed that patients’ and their families felt ‘scared’, ‘invisible’ and ‘not involved’ in the assessment and decision-making process. This was likely due to time not being taken to explain it in their preferred language. Figure 1 depicts the emotions described by patients’ and their families as they journey through hospital when presenting with breathing difficulty.

{kind=link}
Emotional mapping analysis of patients’, presenting with breathing difficulties and their families who prefer to communicate in a language other than English.
The results of our exploratory study highlight the need to improve our services for patients who prefer communication in an alternative language. We learnt that there is a significant demand for our services to be provided in a range of languages and failing to do so can result in children and families feeling uncertain and confused. Unfortunately, the findings in our service are consistent when reviewing the literature on language barriers within the UK and internationally.2
To address these findings, we implemented a low-cost and small-scale intervention to provide personalised asthma care plans that are bespoke to the child’s health needs and in their preferred language.3 We are currently piloting this in Arabic. Our rationale for this is:
Respiratory presentations are common and asthma-related deaths may be preventable with improved management and patient education.
Arabic is the second most preferred language within our trust in both inpatient and outpatient settings.
We aim to expand this initiative to other conditions and languages.
In conclusion, we learnt that language barriers are commonly experienced by patients and can negatively impact their experience and outcomes. However, we believe that this obstacle can be eliminated through appropriately designed healthcare services—we hope that our low-cost intervention can provide an example of this.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and adhered to Imperial Healthcare NHS Foundation Trust audit guideline and protocols. Participants gave informed consent before taking part in the study and all information is annoymosied. External ethics approval was not required for the project.
Footnotes
Contributors All authors confirm that they are responsible for the study conception, design, data collection, analysis, interpretation of results and manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.