Article Text

Abstract
Background Neonatal hypothermia has been widely regarded as a major contributory factor to neonatal mortality and morbidity in low-resource settings. The high prevalence of potentially preventable hypothermia today urges an investigation into why neonates still become hypothermic despite awareness of the problem and established thermal care guidelines. This study aimed to explore the gaps in knowledge and practices of neonatal thermal care among healthcare workers in low-resource settings.
Methods A cross-sectional, questionnaire-based survey was performed online among healthcare workers in low-resource settings. We applied a purposive and snowballing sampling method to recruit participants through a two-round international online survey. Questionnaires were developed using themes of neonatal thermal care extracted from existing neonatal care guidelines.
Results 55 neonatal care professionals participated in the first-round survey and 33 in the second. Almost all participants (n=44–54/55) acknowledged the importance of the WHO’s warm chain to keep a neonate warm. However, fewer participants (n=34–46/55) responded to practice them. When asked about cold stress, defined as a condition in which neonates are below optimum environmental temperature and using more oxygen and energy while maintaining normal body temperature, 15 out of 55 participants answered that checking extremity temperatures by hand touch was useless. Some participants reported concern about the extremity temperature’s inaccuracy compared with core temperature. Opinions and preferences for rewarming methods differed among participants, and so did the availability of warming equipment at their institutions.
Conclusion An inadequate understanding of cold stress underestimates the potential benefits of extremity temperatures and leads to missed opportunities for the timely prevention of hypothermia. The current thermal care guidelines fail to highlight the importance of monitoring cold stress and intervening before hypothermia occurs. Therefore, we urge introducing the concept of cold stress in any neonatal thermal care guidelines.
- neonatology
- nursing
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In low-resource settings, hypothermia has been widely regarded as a major contributory factor to neonatal mortality and morbidity.
A high prevalence of neonatal hypothermia is regularly reported in low-resource settings even though it can be prevented with appropriate thermal care.
Hand touch to detect hypothermia is recommended as a screening tool in community settings where thermometers are not available.
WHAT THIS STUDY ADDS
The neonatal physiological defence mechanism against cold stress is not well understood among healthcare workers in low-resource settings.
Healthcare workers underestimate the potential benefit of extremity temperatures checked by hand touch as an early indicator of cold stress before hypothermia occurs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Introducing the concept of cold stress in any neonatal thermal care guidelines is recommended.
Extremity temperatures must be checked by hand touch as an early indicator of cold stress before hypothermia occurs.
Introduction
Each year, 2.4 million neonates die, 80% in sub-Saharan Africa and South Asia1 and 99% in low-income and middle-income countries.2 Hypothermia has been widely regarded as a major contributory factor to neonatal mortality and morbidity in low-resource settings, referring to settings where healthcare systems do not meet the minimum standards set by the WHO.3 Numerous studies have proved that hypothermia is associated with prematurity,4–6 infection7 and asphyxia,8 9 which are considered the three major causes of neonatal mortality.10 WHO defines neonatal hypothermia as a body core temperature below 36.5°C.11 A high prevalence of neonatal hypothermia is regularly reported, especially in low-resource settings.5 6 12
Neonates, particularly preterm and low-birth weight infants, cannot maintain their body temperature without an appropriate thermal environment.13 In the mid-1900s, researchers demonstrated improved neonatal survival by using warming devices to provide adequate thermal care.14 15 WHO first published thermal care guidelines to inform healthcare workers at all levels about neonatal thermal care in 1993.16 The guidelines recommend 10 codependent procedures, called the ‘warm chain’, to minimise heat loss and prevent hypothermia in neonates at birth and thereafter.11 The warm chain consists of (1) a warm delivery room, (2) immediate drying, (3) skin-to-skin care, (4) early initiation of breast feeding, (5) delayed bathing and weighing at birth, (6) appropriate clothing and bedding, especially the use of a hat,17 (7) keeping mother and neonate together, (8) warm transportation, (9) warm resuscitation and (10) awareness and training.
Regarding rewarming hypothermic neonates, the WHO guidelines recommend using external heat sources such as radiant warmers, heated mattresses and closed incubators. If no equipment is available, skin-to-skin care is recommended for clinically stable neonates.11 For clinically unstable hypothermic neonates, rewarming and maintaining normal temperature remain a challenge when no equipment is available.18
To assess the thermal status of the neonate, axillary or rectal temperature is commonly measured.5 19 However, this proxy for core temperature detects established body temperature only. It gives no clue about the dynamic physiological efforts such as peripheral vasoconstriction or metabolic heat generation to maintain core temperature under conditions called ‘cold stress’.20 In physiological terms, cold stress is a condition in which the environmental temperature is below the lower critical temperature to provide thermal neutrality.21 Although the importance of monitoring foot and hand temperatures for early detection of cold stress before core temperature drops has been emphasised over the decades,22 23 this simple means remains undervalued and recommended only as a second choice in clinical practice.11
Most neonatal hypothermia is preventable because it is due to inadequate thermal care rather than a complication of prematurity.24 25 The high prevalence of potentially preventable hypothermia today urges an investigation into why neonates still become hypothermic despite awareness of the problem and the established WHO thermal care guidelines. This study aimed to explore the gaps in knowledge and practices of thermal care among healthcare workers in low-resource settings.
Methods
Study design and participants
A cross-sectional, questionnaire-based survey was performed online among healthcare workers in low-resource settings. We applied a purposive and snowballing sampling method to recruit participants through a two-round international online survey. The first round explored the general themes of neonatal thermal care, whereas the second round looked at the narrow-scoped themes identified from the results of the first round. The survey was disseminated to physicians, nurses and midwives in neonatal care at all levels of institutions in low-resource settings internationally by e-mails and social networks (Facebook and LinkedIn). Survey participants were encouraged to spread the survey to their contacts. We also invited healthcare workers in neonatal care from high-resource settings with extensive clinical experience in low-resource contexts to generate more diverse opinions. As this study was a descriptive study using purposive and snowballing sampling, there was no agreed sample size.26 Therefore, we aimed for a sample size of 30, which was realistic to achieve with participants from low-resource settings or who had worked there. Healthcare workers, who were invited for the first round, were invited for the second round.
Development of the online survey
The questionnaire for the first-round survey was developed using themes of neonatal thermal care extracted from existing neonatal care guidelines, including the WHO thermal care guidelines.11 27 28 The questionnaire for the second-round survey was developed based on themes that emerged from the first-round survey results. We provide the questionnaires for both rounds of the survey in online supplemental material. The survey included multiple-choice questions and Likert rating scales, supplemented with free-text answers. The questionnaires for both rounds were developed with four neonatal care experts. Piloting of the questionnaires was undertaken in collaboration with two healthcare workers. The survey was developed in English, translated into French and administered anonymously via Google. Both surveys took approximately 10 min to 15 min to respond to. The data from the survey were collected between February and June 2021. Data were collated and summarised using descriptive measures with Microsoft Excel V.2018 (Redmond, Washington).
Supplemental material
The following definitions were used within the questionnaire.
Cold stress: a condition in which neonates are below optimum environmental temperature and using more oxygen and energy while still maintaining normal body temperature21
Core temperature: rectal or axillary temperature11
Extremity temperature: foot or hand temperature.20
Results
Demographic characteristics of participants
Out of 79 neonatal care professionals contacted, 55 completed our questionnaire in the first-round survey (response rate=69.6%, table 1): 25 medical doctors (45%), 16 nurses (29%) and 11 midwives (20%); 22 participants (40%) were from South and Southeast Asia, 21 (38%) from Sub-Saharan Africa and 3 (5%) from Middle East. In the second round, 33 healthcare workers participated (response rate=60%): 21 medical doctors (64%), 2 nurses (6%) and 8 midwives (24%); 18 (55%) of them were from Sub-Saharan Africa, 6 (18%) from South and Southeast Asia and 9 (27%) from other countries.
Characteristics of participants
Monitoring of temperature
Most participants (n=41/55) answered that the quality of temperature monitoring at their institutions was excellent or good. When asked about cold stress, 27% (n=15/55) of participants reported that checking the foot or hand temperature by hand touching the skin of the feet or hand was useless or extremely useless (figure 1). A higher percentage of medical doctors and clinical officers reported so (39%) compared with nurses and midwives (15%). Six participants (three medical doctors, two midwives and one clinical officer) commented about the inaccuracy of extremity temperature compared with rectal or axillary temperature. Most participants (n=28/33) agreed on the nurse’s and midwive’s capability to detect cold extremity temperatures by hand touch, whereas fewer participants (n=20/33) agreed on the mother’s and family member’s capability to do so.
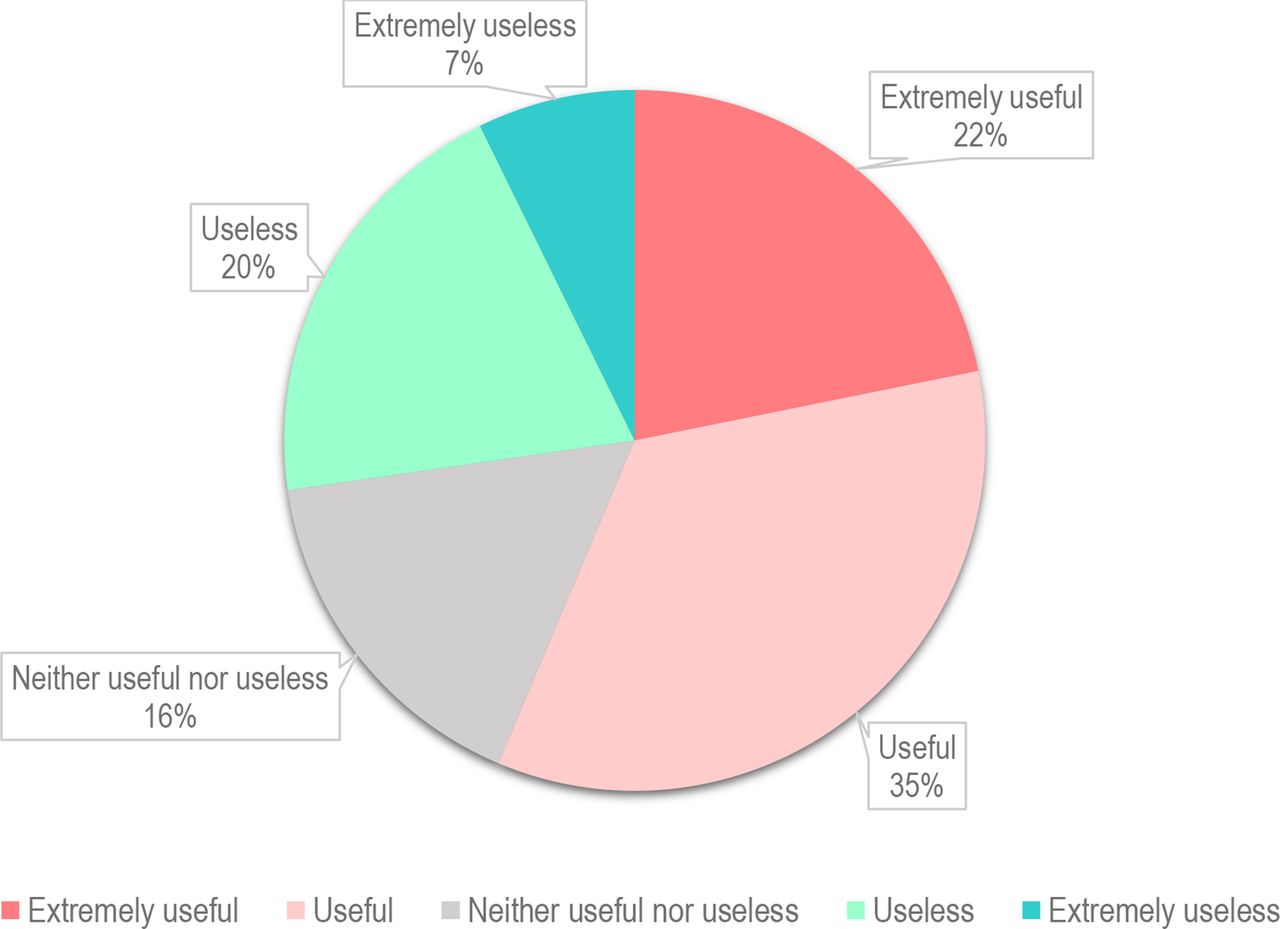
The usefulness of hand touch measurement of foot and hand temperatures.
Prevention of hypothermia
Figure 2 summarises reported acknowledgements on the importance of the WHO warm chain and their reported practice. Almost all participants agreed on the importance of the 10 producers of the warm chain. They reported that these procedures were performed relatively well within their institution. Very few answered that these measures were practised either poorly or extremely poorly. However, the positive responses (strongly agree or agree) regarding the importance of knowledge exceeded those of the perceived quality of practice (excellent or good), especially of skin-to-skin care (% difference=25%), awareness/training (% difference=20%), delayed bathing and weighing at birth (% difference=18%) and warm transportation (% difference=17%). Without exception, all procedures scored lower for practice than knowledge.

Acknowledged the importance and quality of the practice of the WHO-10 procedures of the warm chain.
Management of hypothermic neonates with warming devices
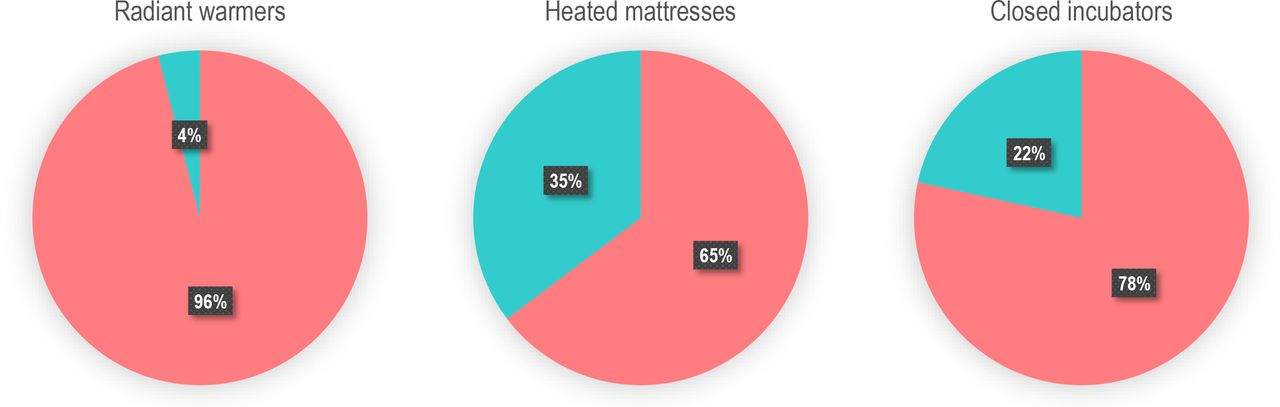
Participants reported that using the following devices is either important or extremely important to treat hypothermic neonates: radiant warmers (n=47/51); closed incubators (n=38/50); and heated mattresses (33/50). The following devices were unavailable in some of the participants’ institutions (figure 3): radiant warmers (n=2/50), closed incubators (n=11/51) and heated mattresses (n=18/51).
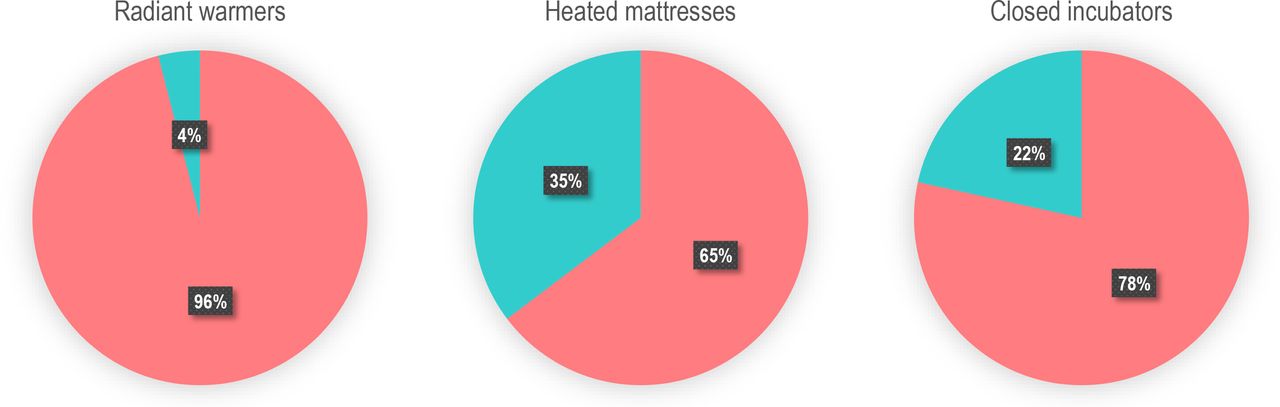
Availability of warming devices.
When asked to assess warming devices (figure 4), most participants answered that closed incubators (n=31/32) and radiant warmers (n=29/32) were considered either effective or highly effective. However, fewer participants (n=22/33) answered so about heated mattresses. Eighty-four per cent of participants (n=26/31) reported that purchasing cost of an incubator was considered expensive and only 29% (n=9/31) thought that a heated mattress was expensive.
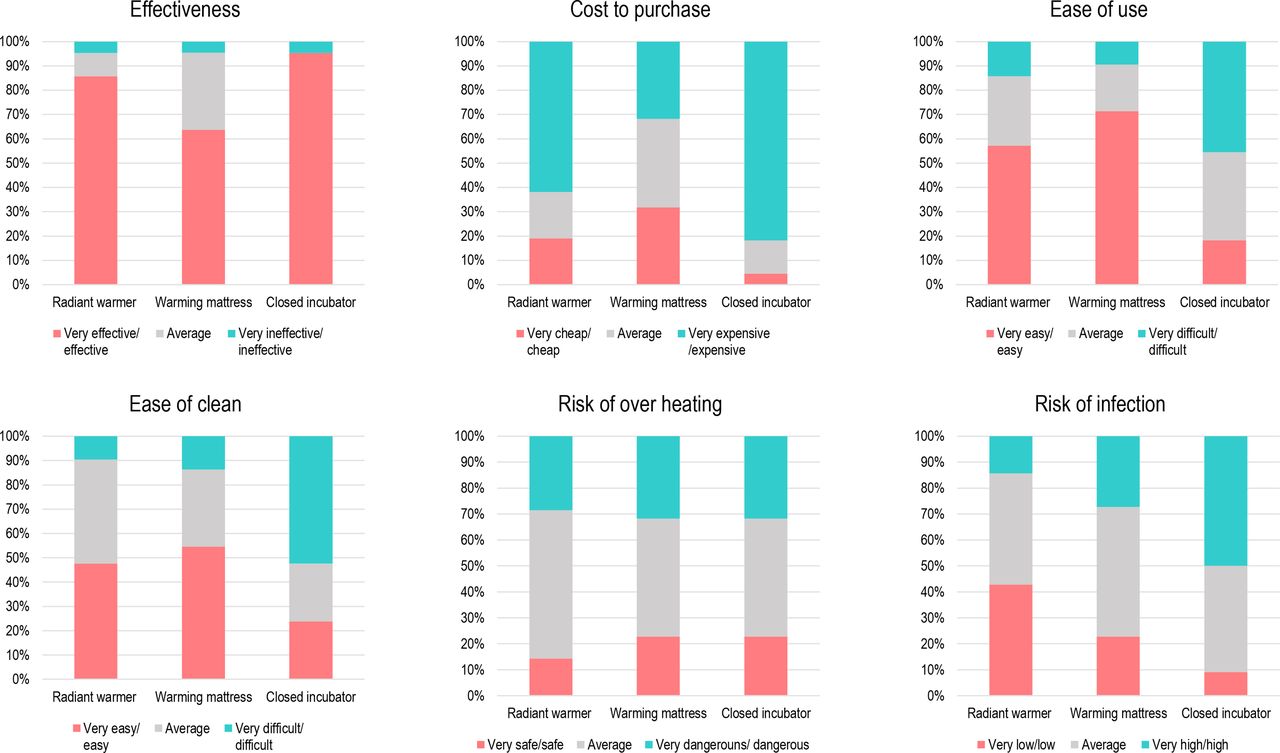
Assessment of warming devices.
In terms of case management, for an example case of a late preterm neonate, with an axillary temperature of 34.0°C and respiratory distress syndrome requiring oxygen, the priority was given by participants to use radiant warmers (n=13/33), followed by closed incubators (n=8/33), skin-to-skin care (n=8/33), heated mattresses (n=3/33) and other methods (n=1/33), considering all the equipment was available (figure 5). Among eight participants who answered skin-to-skin care as their method of choice, six nevertheless answered that they would use warming devices instead in real life. On the other hand, three participants, who preferred either radiant warmers, heated mattresses or closed incubators in theory, would use skin-to-skin care at their institution.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Choice of a warming method for rewarming.
Discussion
Knowledge gaps in the neonatal defence mechanism against cold stress
As the most prominent finding, we identified lacking knowledge on the importance of extremity temperatures as an early indicator of cold stress before hypothermia occurs. Unfortunately, the definition of cold stress is often confusingly reported in the literature merging its physiologic definition (without actual hypothermia) and mild hypothermia, two metabolically different states.20 Even though the physiologic definition of cold stress was provided within the questionnaires, core temperature was considered more valuable than extremity temperature as an indicator of cold stress. Several comments, too, demonstrated indiscriminate understanding of physiologic cold stress and hypothermia.
In the neonate, cold stress triggers vasoconstriction, leading to metabolic heat production with major substrate and oxygen consumption and may limit other organ functions.29 Hypothermia occurs only when this metabolic surge is exhausted. Vasoconstriction is most pronounced in the extremities,20 leading to acrocyanosis, decreased peripheral perfusion and lowered temperature.11 Clinical detection of cold stress with a difference between core and extremity temperatures is widely used by neonatologists worldwide. The literature reports that human temperature sensing in non-diabetic adults can detect smaller than 1°C difference,30 which is appropriate for detecting physiologic cold stress in neonates.20 In deed, Singh et al31 reported the precision of the hand touch method as evaluated by three paediatricians at three sites (abdomen, foot and forehead) where temperatures <36.5°C were accurately detected by hand touch. Extremity temperatures checked by hand touch, an inexpensive, easily available clinical monitoring tool, is an early and sensitive parameter to detect cold stress while core temperature is still normal.32
Thermal care guidelines, including the WHO guidelines, do not distinguish between cold stress and hypothermia.11 27 28 We believe that physiologic cold stress should be considered the established disease because the overrun metabolic capacity hampers critical postnatal adaptational processes relying on energy and oxygen. When cold stress is detected, immediate intervention should be the re-establishment of a thermoneutral environment in which neonates do not consume excess oxygen and energy for thermoregulation. On the other hand, when hypothermia is detected, the intervention should focus on both rewarming the neonate and re-establishing the thermoneutral environment. Since cold stress and hypothermia are clearly two different metabolic conditions, the cursor should be placed between them.
Gaps between knowledge and practice of preventing neonatal hypothermia
When WHO published the thermal care guidelines, the high prevalence of neonatal hypothermia resulted more from the lack of knowledge than equipment.16 This study showed that the importance of the WHO warm chain was well acknowledged, but there is room for improvement in its practice. Deng et al33 conducted a study to explore the factors impacting nurses’ knowledge, perceptions and practice related to skin-to-skin care in neonatal intensive care units in China. They found that most nurses acknowledged the benefits of skin-to-skin care, but depth of knowledge and awareness were inadequate, thus affecting their performance in supporting skin-to-skin care. We feel that an in-depth knowledge of the difference between cold stress and hypothermia will significantly fill this gap between knowledge and practice. However, knowledge alone does not assure practice. Deng et al33 also reported that the nurses perceived increased workloads with significant time consumption of skin-to-skin care implementation as a disadvantage. A proper facility setup and sufficient human resources are necessary for healthcare workers to practice thermal care based on their knowledge.34
Lack of guidance on equipment to rewarm hypothermic neonates
Unlike preventive measures, opinions on rewarming methods differed among participants. Some preferred radiant warmers and others preferred closed incubators. Many participants were uncertain about the effectiveness of heated mattresses. Thus, they preferred skin-to-skin care to heated mattresses for rewarming even in clinically unstable neonates.
Many of these choices may directly result from the availability of these technical devices in the participants’ working environment and the practical experience. The difference between theoretical and practical preferences warrants the careful implementation of warming devices to avoid using complex and costly equipment where lower technology may be sufficient, especially when it limits skin-to-skin care.
Most participants agreed that closed incubators were expensive to purchase even though they were considered effective, which may explain the low availability of closed incubators in their institutions. WHO warns that closed incubators may be more of a hazard than a benefit to the neonate and should only be used in hospitals where skilled personnel can run, maintain and repair them and where a reliable electricity supply is warranted.11 Based on the responses from our questionnaire, the reasons why heated mattresses remain largely unavailable in many institutions appear to be the perceived uncertainty of their effectiveness. Affordable, robust and easy-to-use warming devices, whatever they may be, must be made available to prevent and treat neonatal hypothermia in low-resource settings. Although there is not a one-size-fits-all approach to rewarming hypothermic neonates, practical guidance for choosing context-adapted warming devices balancing effectiveness, safety and affordability is necessary.
Limitations
Although closed questions were time efficient and easier to analyse statistically, they limited the range of participant responses. Another limitation was a low diversity in participants due to the difficulty in recruiting, thus possibly limiting the generalisability of the results. Finally, due to the voluntary nature of participation in the survey, the response rate of the second survey by participants of the first survey was low, and the questionnaire lacked some answers which may weaken the validity and reliability. Providing denominators where applicable, however, may have improved them.
Conclusions
An inadequate understanding of cold stress underestimates the potential benefits of extremity temperatures and leads to missed opportunities for the timely prevention of hypothermia. The current thermal care guidelines fail to highlight the importance of monitoring and detecting cold stress and intervening before hypothermia occurs. Therefore, we urge introducing the concept of cold stress and the hand touch method to check extremity temperatures to detect cold stress before hypothermia occurs in any neonatal thermal care guidelines. The full potential, effectiveness and feasibility in monitoring thermoregulation of the neonate remain to be more broadly investigated in low-resource settings, though.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The University of Geneva and the Cantonal Commission for Research Ethics exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the following individuals for their contribution: Dr. Ahmed Ilyas Sh, Ms. Elizabeth Anyango Walumbe, Dr. François Niada, Dr. Kuissi Kamgaing Eliane, Mr. Mathiang Majok Deng, Dr. Nadia Lafferty, Dr. Sayori Kobayashi, Dr. Sweet C Alipon and Mr. Serge Dzeukou. We also thank all anonymous contributors to the questionnaire.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MK: Conceptualisation, methodology, data collection and analyses, writing—original draft preparation, reviewing and editing. REP: conceptualisation, methodology, data analyses, writing—reviewing and editing. VJ, FR-M and GBP: data analyses, writing—reviewing and editing. REP is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.