Article Text

Abstract
Objective We established a paediatric demand management (PDM) service in our paediatric department in 2017. The aim of this consultant-delivered service is to manage referrals more efficiently by providing active triage of all referrals, daily rapid access clinics and easily accessible advice for primary healthcare professionals. This study presents an evaluation of this service.
Design Mixed-methods service evaluation with analysis of data for every contact with the PDM service over a 2-year period. For each patient, the method of contact, reason for contact, presenting complaint and triage outcome were recorded. Feedback from general practitioners (GPs) and patients was gathered.
Results Data were analysed for 7162 patients. More than a quarter (2034; 28%) of all referrals were managed with advice only. Of the 4703 outpatient clinic referrals, 1285 (27%) were managed without a clinic appointment. More than half (54%) of the requests for paediatric assessment unit (PAU) admission were managed alternatively, typically with advice only or a rapid access clinic appointment. This has reversed the increasing trend of PAU admissions from primary care of preceding years. Financial analysis suggested the avoidance of these clinic appointments, and PAU admissions provided a substantial cost saving.
Conclusions Our results indicate that the PDM service has succeeded in reducing unnecessary hospital attendances by managing patients more effectively and strengthening partnerships with primary care. The service has received overwhelmingly positive feedback from GPs. This service could be replicated in other Trusts and developed in the future to facilitate further management of paediatric cases in a primary care setting.
- health services research
- qualitative research
- data collection
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Increasing demand on acute and elective paediatric services throughout the UK is unsustainable.
There is a need for better integration between primary and secondary care to ensure that paediatric patients are managed effectively in a community setting where appropriate.
Few studies have evaluated the impact of a combination of interventions aimed at alleviating unnecessary paediatric hospital activity.
What this study adds?
Our new consultant-led triage service facilitated successful management of 364 (54%) patients referred for same-day attendance with advice or rapid access clinic appointment.
Providing direct access to the paediatric demand management consultant during office hours led to the management of 27% of all outpatient referrals without face-to-face contact.
Primary care feedback on this new integrated pathway was overwhelmingly positive.
Introduction
Escalating demand on elective and non-elective paediatric services is of national concern. It is generating unsustainable pressure on medical, nursing and administrative staff; poor patient experience; and increasing cost for commissioners.1–3 National Royal College of Paediatrics and Child Health (RCPCH) standards emphasise increased consultant input and collaboration of primary and secondary care services to reduce unnecessary paediatric attendances and outpatient reviews while ensuring children are managed effectively in the community.4 5 Attempts to achieve this in the UK include implementation of consultant-led email and telephone advice lines, acute assessment units and rapid access clinics2 3 6; however, these mainly target same-day admissions only. Evidence on their effectiveness is variable and limited to isolated interventions.2 6–8 Few studies have evaluated combined initiatives targeting both acute and outpatient paediatric referrals.6 At the time of writing, during the COVID-19 pandemic, virtual consultations and community-based management have replaced many face-to-face paediatric reviews. This reinforces the need to explore alternative out-of-hospital integrated care pathways.
The paediatric demand management (PDM) service was established at the Royal United Hospitals Bath NHS Foundation Trust in January 2017. The aim of the service is to manage both inpatient and outpatient paediatric referrals more efficiently by consultant-led triage of all referrals, daily rapid access clinics and provision of direct advice and guidance to primary healthcare professionals. We proposed that this new service would facilitate supported management of a significant number of paediatric hospital referrals in primary care. This review presents an evaluation of our PDM service.
Methodology
Setting
The Royal United Hospital (RUH) is an average-sized district general hospital providing secondary paediatric care to a population of approximately 80 000 children. Inpatient services comprise a 33-bed children’s ward and a paediatric assessment unit (PAU), open from 08:00 to 20:00 daily. The majority of inpatients are admitted from PAU aside from overnight admissions or direct admissions to the ward where an overnight stay is anticipated. PAU admissions are predominantly referred by primary healthcare professionals (mostly general practitioners (GPs)). Other sources of referrals include the emergency department (ED) and a small number of self-referrals of patients with long-term health conditions.
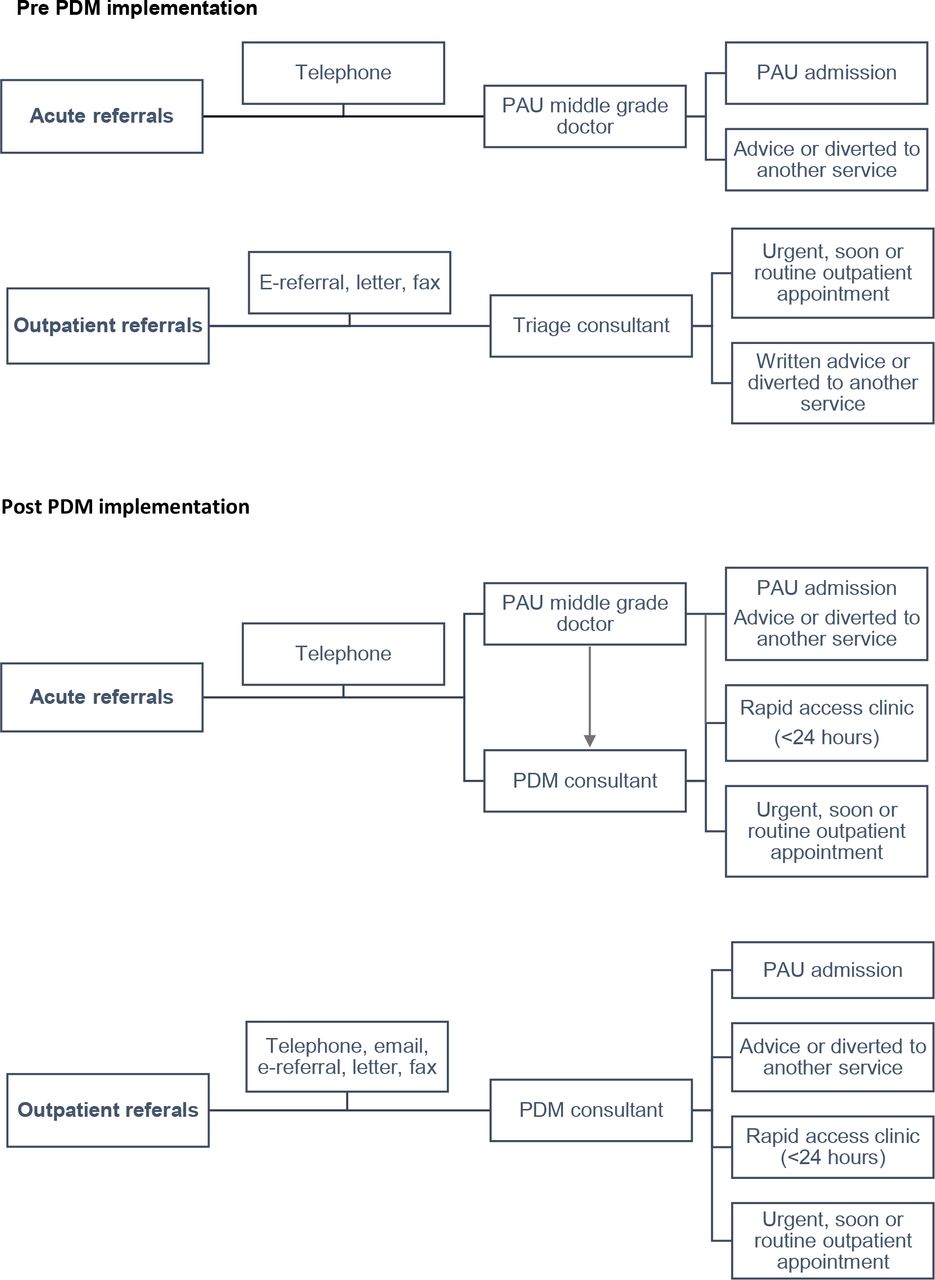
Prior to the introduction of the PDM service, children were referred to PAU via the on-call middle grade doctor with very few diverted or avoided. Outpatient paediatric referrals were communicated by letter, fax or electronic referral system, without any prior discussion with the paediatric team. The triage consultant was also the consultant on acute service with no dedicated time to invest in alternative referral management (figure 1).
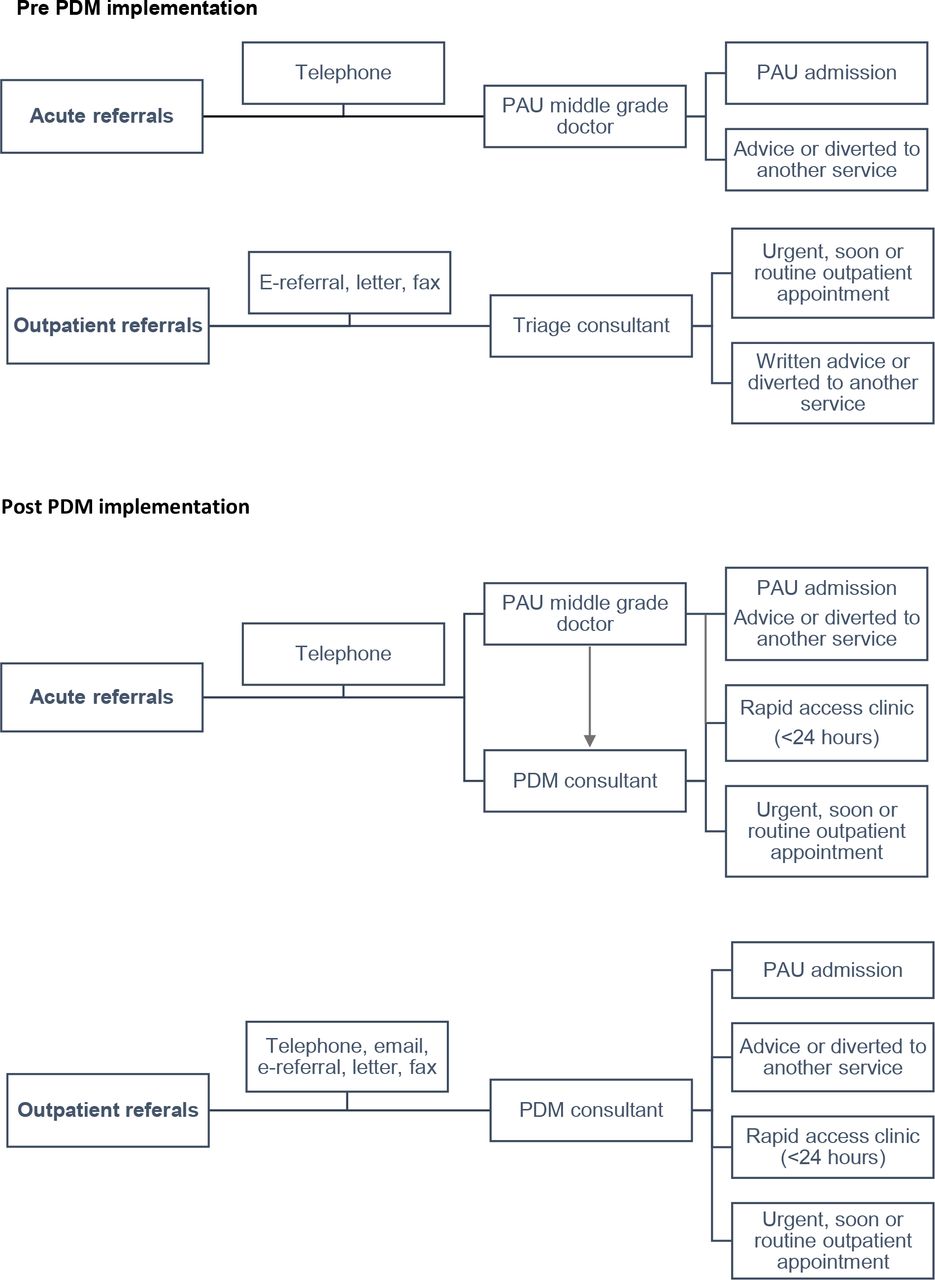
Referral pathways and outcomes before and after PDM implementation. PAU, paediatric assessment unit; PDM, paediatric demand management.
Intervention
The PDM service was initiated as a 2-year pilot project in January 2017, following approval and financial support from BaNES and Wiltshire clinical commissioning groups (CCGs). Individual elements constituting PDM were chosen based on RCPCH recommendations4 5 and perceived success in other UK paediatric departments. Some of these were trialled previously by the department (consultant mobile and ad hoc clinics) but deemed unsuccessful due to the lack of dedicated consultant availability for the additional responsibilities. A locum consultant was therefore appointed in January 2017, enabling one general paediatric consultant to be allocated to the PDM service each weekday. This role was rotated through six consultants, with two covering the majority of the rota. The PDM consultant’s daily responsibilities included the following:
Telephone advice and guidance to primary care healthcare practitioners, ED, paramedics, RUH consultants, and Child and Adolescent Mental Health Services psychiatrists via a dedicated consultant mobile (09:00 to 17:00).
Providing advice and guidance via a dedicated email address, including reviewing photographs, ECGs and videos.
Daily rapid access clinics including same-day appointments.
Active triage of all outpatient paediatric referrals, supporting management of patients in primary care if appropriate.
Referral pathways and outcomes before and after implementation of PDM are outlined in figure 1. The PAU middle grade doctor continued to receive the majority of same-day admission referrals but could redirect these to the PDM consultant where admission avoidance was anticipated. Discussion of acute referrals was also extended to paramedics after implementation.
Design
We performed a mixed-methods service evaluation of all patients referred and triaged through the PDM service over a 2-year pilot period. Our aim was to review use of the service and describe its impact through referral outcomes, admission and referral avoidance, primary care and patient feedback, and financial analysis.
Method
Data for every contact with the PDM service were collected prospectively on a departmental database to enable service evaluation and regular reporting to commissioners. We analysed these data and quantified the following outcomes:
Method and reasons for contact.
Referral outcomes.
Management of 10 most common presenting complaints.
GP and patient feedback.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our study.
Results
Data collated for 7162 patients managed via the PDM service over a 2-year period from January 2017 to January 2019 were reviewed.
Method of contact
Electronic outpatient referrals (2254; 31.5%) and telephone calls (2252; 31.4%) were the most used means of contact, followed by outpatient referral letter (1312; 18.3%) and email (1014; 14.2%). A small proportion of referrals (69; 1%) were redirected by the PAU doctor.
Reasons for contact
The most frequent reason for contacting PDM was a routine paediatric outpatient referral (3183; 44.4%). Referrals for an urgent (within 2 weeks) or soon (within 6 weeks) clinic appointment constituted 1520 (21.2%) contacts. A significant proportion of contacts were for advice only (1592; 22.2%), mostly via telephone or email. The remainder included referral to PAU (676; 9.4%) and requests to expedite a pre-existing referral (190; 2.7%) (figure 2).
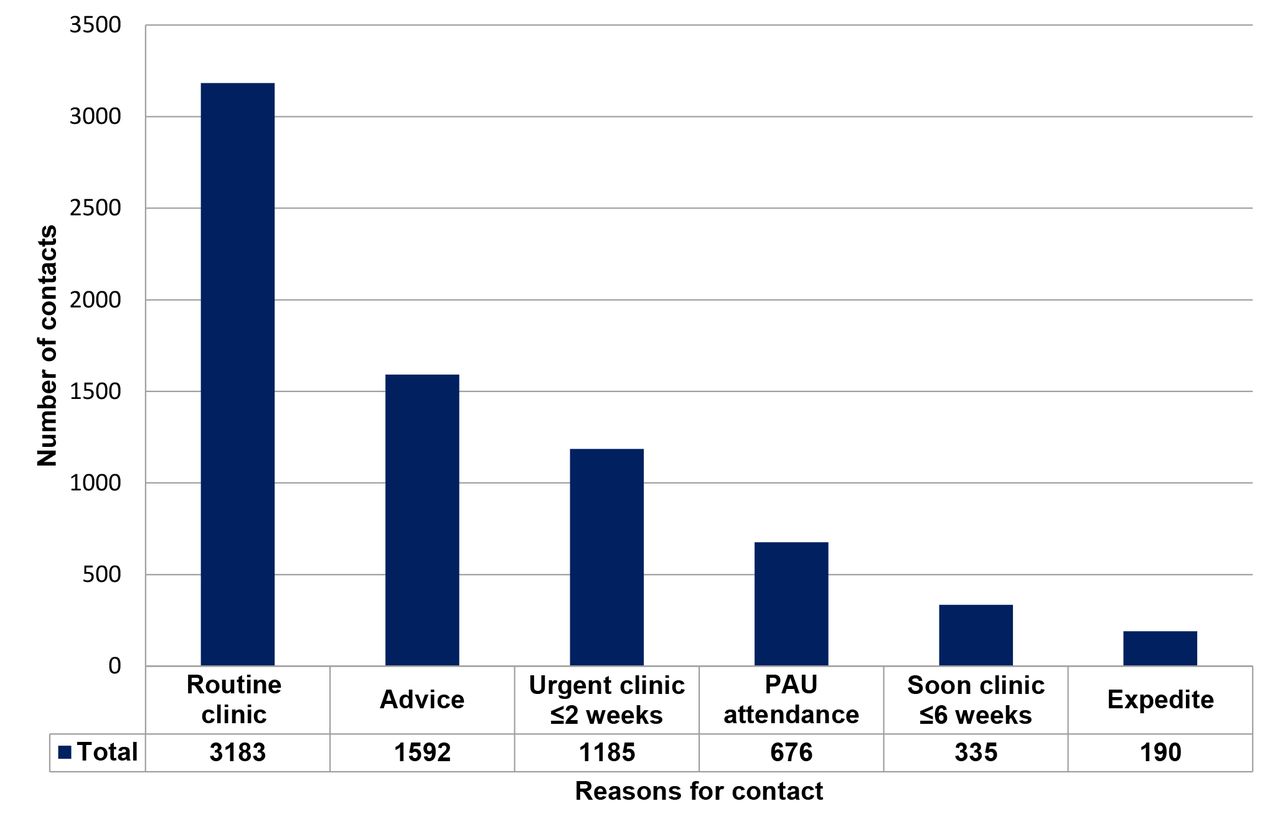
Reasons for contacting the paediatric demand management service. PAU, paediatric assessment unit.
Outcomes of referrals to PDM
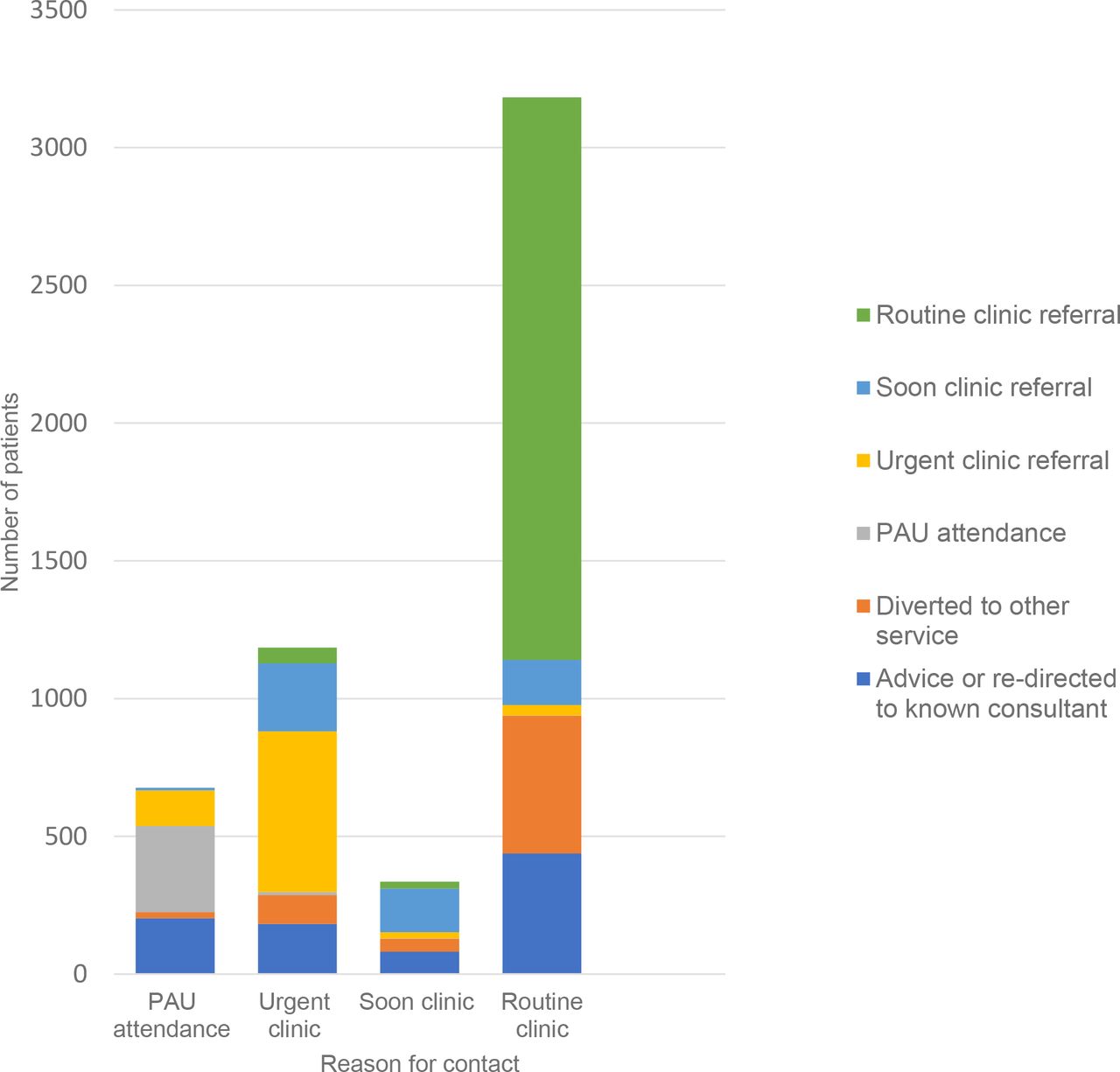
Twenty-eight per cent (2034) of all referrals via PDM were managed with advice only. A further 814 (11.4%) were diverted towards a more appropriate service, including hospital or community-based allied healthcare professionals (eg, physiotherapy) or another hospital specialty. Just over half (53.8%) of the referrals to PAU were managed alternatively, resulting in admission avoidance in 364 patients. Of those cases, 195 (53.6%) were given advice and 130 (35.7%) were offered a rapid access clinic appointment (figure 3). Year 1 pilot data for GP-referred admissions to PAU demonstrated a 10% reduction compared with a year-on-year increase for the 5 preceding years (average 17% per year). Year 2 demonstrated a slight (2.5%) increase in admissions, but still a significant contrast with the previous trend.

Paediatric demand management service referral outcomes based on reasons for contact. PAU, paediatric assessment unit.
Approximately half of the requests for an urgent clinic (583; 49.2%) or soon clinic (159; 47.5%) were accepted; however, 415 (27.3%) were managed without face-to-face contact. The majority of routine clinic referrals (2043; 64.2%) were deemed appropriate, with a small proportion (203; 6.4%) being offered an earlier review (PAU attendance, urgent or soon clinic). The remainder were managed alternatively, 483 (13.8%) with advice or redirecting the issue to their known consultant and 499 (15.7%) signposted to another service. In total, 1285 (27.3%) of all 4703 outpatient referrals were managed without a clinic appointment (figure 3).
Most common presenting complaints
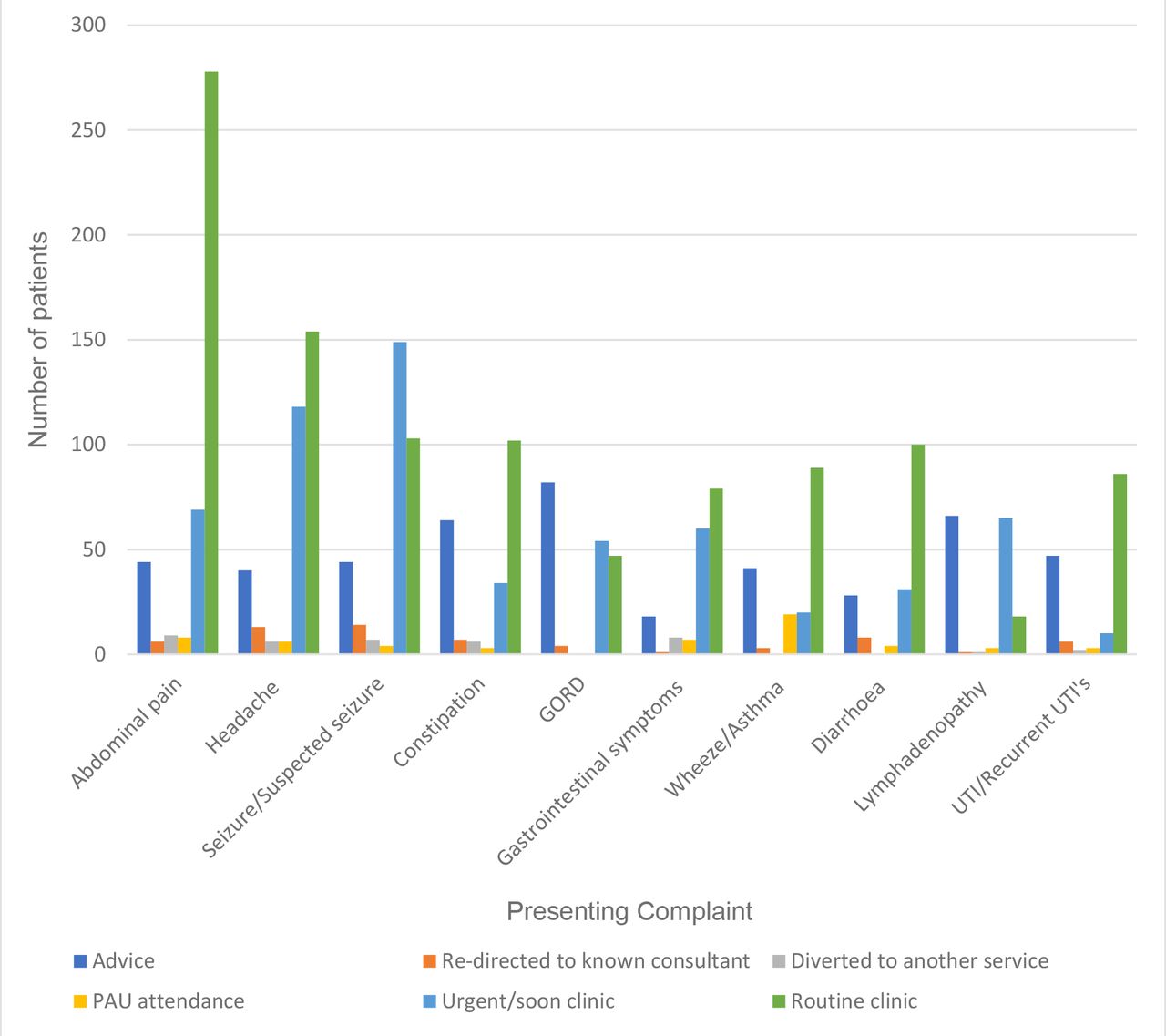
Abdominal pain was the most common presenting complaint in this patient cohort, constituting 414 referrals. The majority of these (278; 67.1%) were allocated to a routine clinic appointment; however, 44 (10.6%) were given advice and 69 (16.7%) were offered an urgent or soon clinic appointment. Referrals for gastro-oesophageal reflux disease (GORD) and lymphadenopathy were managed with advice only in almost half of the cases. Patients referred with confirmed or suspected seizures were most commonly offered an urgent or soon clinic appointment. For 6 of the top 10 presenting complaints, at least 25% of referrals were managed remotely (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Paediatric demand management referral outcomes for the 10 most common presenting complaints. GORD, gastro-oesophageal reflux disease; PAU, paediatric assessment unit.
Primary care feedback
Invitations to complete an online survey regarding usage and feedback on the PDM service were sent to all local GP practices 6 months into the pilot, and the email auto-reply contained a survey link. Seventy-six responses from 37 GP practices were received. Respondents reported usage of multiple communication channels: telephone, 54 (71.1%); email, 47 (61.8%); letter, 14 (18.4%); and e-referral, 15 (19.7%). The majority of contacts were managed with advice only (46; 60.5%). In 27 (35.5%) cases, the patient was seen more urgently than expected, whereas in 8 (10.5%) cases they were seen less urgently than expected. Feedback suggested very high satisfaction rates, with 75 (98.7%) respondents stating they were ‘quite likely’ or ‘very likely’ to use the telephone and/or email service again and 71 (96%) reporting satisfaction with the opinion given. The majority (46; 61.4%) of the respondents agreed that their contact with PDM would change how they manage a patient in the future. The 48 free-text responses were overwhelmingly positive (box 1). Consultants rotating through the PDM role similarly reported satisfaction from offering a more flexible, higher quality service, enabling the consultant on acute service to devote his or her time solely to inpatient work and urgent admissions.
Examples of free-text comments from GP user experiences of demand management
‘Saves us and patients (and hopefully hospital) a lot of time and improves care. Consultants always really helpful and even do some teaching at the same time with us. This is amazing because we can then cascade this to the other GPs at the practice to influence ongoing care’
‘Used the telephone advice line when urgent appointment seemed to go missing. even emailed in a video of a suspected seizure in a patient which was reviewed by two consultants within 24 hrs and outpatient appt/long wait avoided for the patient. I hope this service can continue its been very valuable’
‘Excellent service as always—find this so convenient and useful, and definitely results in fewer referrals from me!’
‘the email service is very much appreciated. It’s a way to communicate in a timely manner, without the interruption of a phone call, it’s also a written record which can be copied and pasted directly into the records. Consultants often include their phone number in case further discussion is needed’
‘Very responsive, very helpful, and as implied above, the advice has given me confidence to manage similar cases myself in the future—this easy process helps avoid letters and delays and I'm sure avoids referrals to clinic’
‘Really useful service, well designed to fit in with how primary care works. Always quickly responded to and has stopped several referrals on the occasions where I have used it’
‘It is very helpful to be able to ask clinical queries and have an expert opinion with the patient and family with us—thank you’
‘Excellent service, all I have spoken to have been friendly and very happy to advise. Also well received by parents who appreciate real-time advice, has certainly reduced their anxiety’
GP, general practitioner.
Patient experience
To evaluate patient experience, a three-question questionnaire was sent via letter and prepaid envelope to 474 families managed via the Demand Management pathway in the first 6 months. We received 30 responses (6% response rate), and no reminders were sent. Twenty-three (77%) expressed satisfaction with the service, two were somewhat satisfied and five were not satisfied. Of those who were not satisfied, comments related to appointment booking issues (2), delay in subsequent investigations (1), being prescribed antibiotics without a consultation (2) and a perceived delay in the process when the child did ultimately need to be seen. These issues were addressed in the following ways:
Contacting the family directly when antibiotics were to be prescribed or other significant change in expectations.
Communicating advice and guidance via letter to both GP and family.
Explaining that if a future appointment became necessary where it was not offered initially, the first contact date would be considered the start of the pathway.
Financial analysis
The traditional Payment by Results policy, whereby reducing departmental activity would result in reduced income, required the implementation of an alternative financial arrangement with our commissioners. During the pilot phase, the CCGs financed the additional consultant time. We agreed that appointments in the rapid access clinic, and calls placed via the PDM consultant, would be tariff-free. During the 2-year pilot period, 2651 clinic appointments and 364 PAU admissions were avoided. This produced estimated cost savings to the CCGs of greater than £400 000 per year, excluding the cost of a new consultant.
Discussion
Our service evaluation indicates that PDM has achieved its aim of facilitating the management of a significant number of paediatric referrals without face-to-face contact. This reversed the year-on-year increase in PAU admissions and outpatient clinic appointments, providing significant annual cost savings to the CCGs. The provision of direct advice and guidance has improved accessibility of paediatric consultants to primary care. This has brought compliance with national standards5 and overwhelmingly positive feedback from GPs, particularly when used with the family still present in the room. This enabled the paediatrician to ascertain additional information first-hand and to communicate advice or management plan directly to the family. Although email advice was sought less frequently, the capacity to share pictures and videos was highly valued and often used as an adjunct to pre-existing referrals. It also allowed time for a more considered response, following a brief literature review, or discussion with a colleague. The benefits of provision of direct advice and guidance to GPs with respect to alleviating paediatric hospital activity have been described in several published studies.8–10 The added educational benefit to GPs is highlighted in our feedback.
Over half of the referrals to our PAU via this service were avoided, which surpassed initial expectations and relieved pressure on the acute workforce. Our results are comparable with a previous study7 in which 50% PAU walk-in attendees were deemed suitable for community management. Unplanned same-day hospital attendances can cause significant disruption and anxiety for families and may expose children to unnecessary investigations, inevitable waits for assessment and reviews, and hospital-acquired infections.9 Empowering GPs to manage cases in the community offers convenience, increased satisfaction and confidence in primary care.10–12
Most of the literature on reducing secondary care activity focuses on acute paediatric presentations. However, we also observed a significant impact on outpatient referrals. Just over a quarter were managed without a face-to-face paediatric review, with either advice or diversion to an appropriate service, ensuring that patients see the right person, first time. Those offered a clinic appointment often had investigations or treatment instigated in advance, avoiding delays in diagnosis and unnecessary follow-up appointments. We lacked follow-up data on patient outcomes, including re-presentation rates for those managed without seeing a paediatrician. However, we have not received any feedback suggesting dissatisfaction since ensuring that GPs and families receive a copy of advice and guidance correspondence.
Analysis of presenting complaints provides an insight into primary care case-mix and incentive for educating GPs, almost half of whom have had no formal paediatric training.5 Eight of our top 10 presenting complaints are included in Birmingham Children’s Hospital top 20 outpatient paediatric conditions,13 implying that these are generalisable. Just under half of the PDM referrals for patients with GORD and lymphadenopathy were managed with advice only. GP feedback implies appreciation of the educational value of direct case discussion, informing future practice, and this could be expanded further in the future.
Strengths of our review include its large sample size and representation of a 2-year time period, reducing potential confounding factors such as seasonal variation and varying staffing levels. We acknowledge that our data are limited to a service unique to our department whose success is dependent on a significant investment in consultant time. However, our cost analysis shows that this investment has been far outweighed by the savings received by CCGs. The response rate from our patient survey was poor in comparison with other studies.12 14 This may reflect differences in methodology; our families were contacted retrospectively by letter on a single occasion.
Following the success of the 2-year pilot project, the PDM service is now permanently embedded in our department. Keys to its success included having a consultant solely dedicated to the role during office hours, good knowledge of available pathways and connecting services, and flexibility in management options. Opportunities for developing this further include establishing partnerships between paediatricians and general practice clusters to improve the quality of community-based management and enabling earlier intervention to avoid future referrals in some cases. This has been successfully implemented as part of the connecting care for children model in North West London,12 boosting confidence in and usage of GP services by parents. Virtual joint telephone and video consultations could be trialled in view of restrictions due to the COVID-19 pandemic. Inclusion of paediatric trainees, who spend a disproportionate amount of time in acute services,15 would also enhance understanding of referral processes and develop capabilities in triage.
Conclusion
Our results demonstrate the impact of restructuring paediatric services to facilitate active triage and flexible management of paediatric referrals from primary care practitioners across different communication channels. They indicate that our new integrated pathway is effective in avoiding a significant proportion of unnecessary paediatric admissions and outpatient referrals by managing patients remotely and has been well received and used by primary healthcare colleagues.
Acknowledgments
We would like to thank Bernadette Burt, senior business analyst at the Royal United Hospital, for her support with data capture and analysis.
References
Footnotes
Contributors LD was the overall supervisor and conceived the idea for the study. HSH and LD analysed and interpreted the data. HSH drafted the manuscript. LD and NW critically reviewed and revised the manuscript. All authors approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.