Article Text

Abstract
Background Over the course of the pandemic, many countries have repeatedly closed schools and shifted schoolchildren to remote learning. However, evidence for negative mental and physiological health consequences of such measures for schoolchildren is increasing, highlighting the need for evidence-based recommendations on how to safely reopen schools. This study aims to assess implementation experiences, acceptability and feasibility of opt-in, at-home SARS-CoV-2 screening using rapid diagnostic tests (RDTs) to facilitate safe face-to-face teaching during a pandemic.
Methods We present data from a prospective study implementing an RDT-based screening programme at a primary school in southwest Germany. In addition to quantitative data collected to assess screening diagnostic yield (number of participants, tests handed out to participants, positive RDT results reported), we conducted qualitative in-depth interviews with participating pupils, parents and school stakeholders to elicit implementation experiences and screening perceptions.
Results The screening intervention was highly accepted and appreciated among participants; no screening-associated positive RDT was reported over the duration of the study. Self-testing at home before coming to school was feasible, but more positive consequences of screening participation (eg, easing of mask mandates) besides a personal feeling of safety would have been appreciated across respondent groups. Participants preferred home-based RDTs over some other measures, particularly mask mandates. Despite the RDTs being licensed as self-tests in Germany, additional training can help avoid mistakes, and ensuring intervention ownership and improving pre-implementation communication can facilitate buy-in.
Conclusions Antigen-RDT-based SARS-CoV-2 screening programmes relying on self-testing at home are a feasible and acceptable supplement to the public health toolbox to facilitate a safe return to face-to-face teaching at schools.
Trial registration number DRKS00024845.
- health services research
- adolescent health
- COVID-19
- qualitative research
Data availability statement
Considering the high public interest in research on COVID-19, qualitative data of participants who have indicated their agreement to this as part of the informed consent procedure can be shared with other researchers. However, to preserve the anonymity of respondents and considering the personal nature of qualitative data, requests will be considered on a case-by-case basis. Please contact the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Efforts to reduce COVID-19-associated school disruption are currently being debated globally to reduce the impact of extended school closures on children’s well-being.
Rapid diagnostic tests (RDTs) for SARS-CoV-2 are reliable and can be performed as self-tests at home.
Although countries have already introduced RDT-based screening programmes to facilitate safe face-to-face teaching, little is known about screening acceptance and experiences.
What this study adds?
Pupils, parents and school staff perceive home-based RDT screening as feasible and less disrupting than other protective measures (eg, mask mandates).
Implementers should communicate early and clearly, and provide a support system for training, troubleshooting, and in case of positive results.
Concerns remain regarding the fidelity of home-based test performance in cases where pupils or parents are hesitant, even when testing is compulsory.
Introduction
To curb infection rates in the context of the COVID-19 pandemic, many countries suspended routine, face-to-face teaching in primary and secondary schools, and—where possible—schoolchildren were shifted to remote learning.1 2 However, as studies outlined the negative effects of school closures on children’s education and health,3 4 and as evidence mounted regarding children’s reduced risk of severe disease progression,5 6 schools began reopening. Amid reopening, debates ensued regarding the nature and content of infection prevention measures. One such measure entailed routine testing via either antigen-based rapid diagnostic tests (RDTs) or pooled PCR testing for SARS-CoV-2.
The proposal to implement large-scale screening efforts at schools was criticised both from an epidemiological perspective (regarding imperfect test performance, especially of RDTs), and from a pragmatic perspective (viewing tests as an unnecessary burden for schoolchildren and their parents).7–9 On the other hand, a study from Great Britain suggested that SARS-CoV-2 protective measures in schools were broadly accepted among schoolchildren and parents, and expansion of routine SARS-CoV-2 testing would be welcomed.10 To the best of our knowledge, there is no evidence available on the perceptions of and experiences with the implementation of testing for entrance screening in school settings, and the effects on compliance with other safety measures (eg, masks).
An in-depth investigation of school-based testing implementation can facilitate evidence-based recommendations for best practices of entrance screening in schools, not only in the context of this pandemic but also for future public health crises. This study responds to calls in the literature to better understand opportunities and challenges for COVID-19 mitigation or prevention strategies in schools. 11–13 We provide insights regarding how RDTs for home-based screening of primary schoolchildren can be implemented, and whether such screening approaches can be a feasible and accepted addendum to the pandemic response toolbox in Germany.
Methods
We conducted a prospective implementation study to assess experiences with and perceptions of introducing in-home RDT-based screening at a primary school in a periurban area of southwestern Germany. Throughout the early pandemic, schools in the region were routinely fully or partly closed, only offering basic face-to-face supervision to children whose parents work in fields classified as essential. Since the beginning of 2021, an increasing number of academics, policymakers, school representatives and parents argued for schools to be reopened with comprehensive screening approaches complementing other hygiene measures.14 15
Responding to calls from policymakers for pilot projects testing the feasibility and acceptability of such screening efforts, our study-based screening was initiated in March 2021. Statewide compulsory screening was introduced for schools in April 2021, informed by findings from pilot projects testing different approaches, including our own study. Figure 1 presents a timeline of study-related processes and the general context.
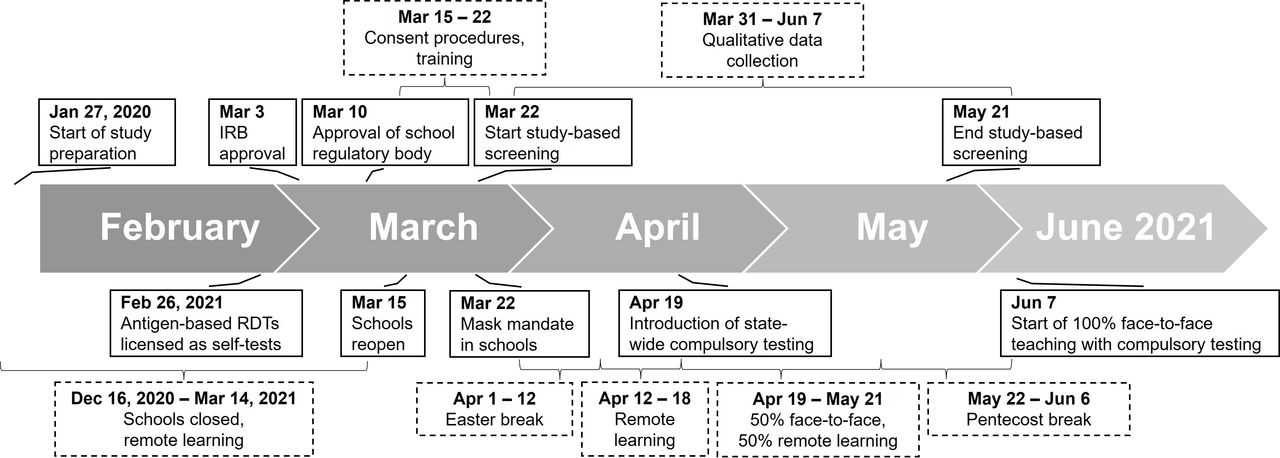
Study processes and the general context. RDTs, rapid diagnostic tests. IRB, institutional review board
Intervention design
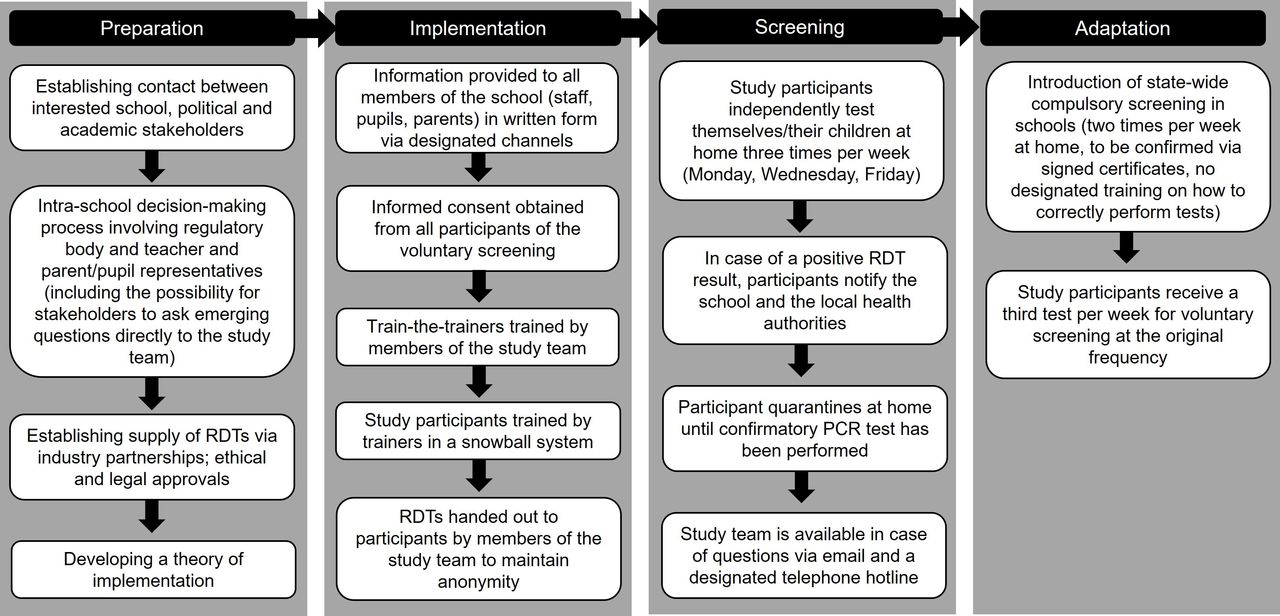
Several schools in the region expressed interest to participate in pilot projects for SARS-CoV-2 screening. We selected one school suited to fill key gaps in the discourse, particularly with regard to setting (periurban) and age of schoolchildren (primary school). The design of the screening intervention was developed in partnership with school stakeholders (figure 2). For each week of screening, pupils and staff members who voluntarily decided to participate in the study received three antigen-based RDTs to be performed independently at home on Mondays, Wednesdays and Fridays. The test used was the STANDARD Q COVID-19 Ag Tests (SD Biosensor, Gyeonggi-do, Korea), an independently validated and WHO-approved SARS-CoV-2 RDT.16 17

Implementation and theory of intervention of the RDT-based screening. RDT, rapid diagnostic test.
We trained members of the school staff and parents who volunteered on how to perform the test, and then trained others in a snowball system. We additionally provided participants with a step-by-step guide on how to perform the test (online supplemental file 1), and we set up telephone and email hotlines that could be contacted in case of screening-related questions. Additionally, the local health authority and local doctors were informed about the study.
Supplemental material
After 4 weeks of screening, compulsory testing was introduced for all schools in the German state of Baden-Württemberg.18 The design of this statewide screening was very similar to the study intervention, with the main difference being only two tests per week and parents having to confirm the test result to the school in writing. No training was offered in the context of the statewide screening. Upon onset of the compulsory screening, all study participants were supplied with one test per week to supplement the two RDTs provided by the state to maintain the original screening frequency.
Data collection and analysis
Quantitative (number of participants, number of tests handed out, and number of tests reported to be positive) and qualitative (in-depth interviews with children, parents and school stakeholders) data were collected over the entire duration of the study; data collection and analysis procedures are outlined in figure 3. All participants provided written informed consent separately for their participation in the screening and, if applicable, when they participated in the qualitative interview. We followed consolidated criteria for reporting qualitative research (COREQ) guidelines19 to report our findings (see online supplemental file 2).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Data collection and analysis. RDT, rapid diagnostic test.
The semistructured interview guides, including questions and further probes (see online supplemental file 3), were developed based on the literature and the study team’s previous experience conducting qualitative interviews on SARS-CoV-2 RDTs in Germany.20 For the qualitative interviews, we chose among 60 parents of 65 pupils who had signalled an openness to participate in an interview, contacting 25 of them via email (and purposefully including them based on residence in larger or smaller villages, and being parents to children from grades 1–4). Half of these emails received a response and we ultimately interviewed 10 parents (stopping early due to data saturation). Reasons for not participating among those who responded to our email invitation but declined or postponed an interview (n=3) included scheduling difficulties and the high workload of managing homeschooling for pupils while working from home oneself. Parents agreeing to be interviewed were asked whether their child would also be open to being interviewed, with 10 children from 9 parents agreeing to participate. School staff and stakeholders were contacted through designated school channels.
Supplemental material
Interviews were scheduled via email and conducted in German on a video call platform of the participant’s choosing. Prior to each interview, the interviewer described the content and purpose of the interview, and participants were invited to ask any questions. Parents and pupils were interviewed together, with the pupil sometimes not being present for the entire duration of the interview. In some cases, respondents’ smaller children were in the same room during the interview. To the best of the interviewer’s knowledge, no other individuals were present.
The lead author (JW), who has graduate level education and several years of experience in conducting qualitative research, conducted all interviews. He acknowledges that working in his country of origin, in close proximity to where he lives, could result in biases, especially in light of being affected by similar COVID-19-associated restrictions and policies as respondents. The interviews on average lasted 45 min (range 24–74 min) and concluded once saturation was reached (for interviews with parents and pupils) or all respondents expressing interest to participate were interviewed (for school stakeholders and staff). JW and MS prepared detailed summaries of each interview, key sections were transcribed verbatim and translated into English.
Qualitative data were analysed drawing on thematic analysis,21 combining inductive (themes emerging from the data) and deductive (concepts derived from the literature) approaches (figure 3). JW iteratively applied the resulting codebook to the entire set of interview summaries, discussing emerging similarities and differences across respondent groups with SAM and CMD.
Patient and public involvement
Members of the school administrative staff and parents of pupils initiated contact with the study staff to express interest for developing a pilot project to assess the feasibility and acceptability of RDT-based screening at schools. Staff and parents were actively involved in the conceptualisation and implementation of the study. To maintain anonymity, school staff were not involved in participant recruitment or data collection. One coauthor (NT) is a parent to two school pupils, was responsible for initiating the study, and also participated in an interview as a key informant.
Results
Study participants
A majority of school staff decided to participate in the voluntary screening (n=21 out of 34, 62%), as well as a majority of pupils and their parents (n=109 out of 186; 59%). After the introduction of the statewide compulsory screening, n=15 (14%) participating pupils did not collect their additional third weekly study-based RDT, indicating that they were screening the state-mandated two times per week. Interviews were conducted with 6 school stakeholders and staff, 10 pupils and 10 parents (9 mothers and 1 father). The study lasted 9 weeks (22 March–21 May 2021). During this time, SARS-CoV-2 incidence in the region initially increased from 106.7 infections per 100 000 inhabitants per week (22 March) to 154.1 (27 April) before it fell to 54.3 by the end of the study-based screening (21 May).22
Over the course of the study, no study-related positive RDT result (neither false positive nor true positive) was communicated to the school or the study team. After the onset of statewide compulsory testing in schools, while the study-based screening was still in place, the school was notified of one case of SARS-CoV-2 in a pupil whose parents had self-reported a negative RDT 1 day prior. No further cases were reported.
Implementation experiences, home-based testing
To highlight implementation processes and experiences, we group themes inductively emerging from the data along the framework of Mc Sween-Cadieux and colleagues (table 1)23 which combines the Consolidated Framework for Implementation Research24 and the Ecological Framework.25 The framework investigates factors influencing intervention implementation across six domains: intervention, individuals, support system, inner setting, outer setting and the implementation process.
Implementation experiences across domains
Intervention
School stakeholders highlighted their key motivations for exploring RDT-based screening as minimising risks of secondary infections and school closures, as well as a hope that screening may lead to other positive consequences (eg, repeal of mask mandates). Some participants voiced concerns regarding screening because it placed an unnecessary burden on children, especially in light of increasing communication at the time that children were not a driver of the pandemic and the perception that children’s physical and mental health was already strained enough by the pandemic. Consequently, a majority of stakeholders appreciated the newest generation of RDTs because they relied on anterior-nasal swabs, which were viewed as less burdensome for those performing the tests in general and children in particular.
A major point of debate entailed whether to conduct screening at home or on-site. School stakeholders and staff predominantly highlighted organisational and infrastructural barriers to school-based screening, including the strain on already limited teaching time, concerns regarding the psychological consequences of a pupil testing positive in school (including potential stigmatisation by peers), and questions regarding teacher accountability. While participants generally acknowledged these concerns, several parents also discussed concerns that not everyone would conscientiously perform the tests at home. This was voiced when testing became compulsory, especially addressing families who initially had decided against study participation.
Individuals
An increased sense of safety was reported as the key motivation for, and consequence of testing across respondent groups for participation in the study and testing in general. Participants also reported a desire to contribute to COVID-19 research, thereby increasing the chance for a timely return to ‘a more normal school routine’ (mother 3). The screening itself was generally appreciated, and a majority of participants described how initial reservations or ‘fear’ (female pupil 3) regarding the tests were alleviated after the first few times, and the screening quickly was integrated into the morning routine ‘like brushing teeth’ (mother 10). Children themselves described RDTs as being much less disrupting or burdensome compared with other measures encountered over the course of the pandemic, in particular compared with mask mandates in schools.
Several participants voiced incomprehension or ‘disappointment’ (school stakeholder 6) regarding the number of families deciding against participation, or recounted frustration when interacting with screening hesitant parents or staff members. Several expressed disappointment regarding the limited consequences of participating in the screening and expected motivation and buy-in of others to increase once testing was seen as having consequences beyond a personal sense of security.
Support system
Participants appreciated offers made by the study team, including telephone and email hotlines, although neither was used during the course of the study. No participant reported interacting with complementary local resources (eg, local health authority or local doctors). The experience of quick notification and confirmatory testing in light of one positive result outside the study was seen as affirming that the support system in place would work.
Most participants appreciated the implemented train-the-trainer system and reported their interactions during the training as reassuring and empowering for when they performed the first RDT with their children, particularly when mistakes emerged during training (eg, moving the test kit around, placing it on an uneven surface, wrong usage of buffer fluid). In a few instances, however, the snowball training system did not work as envisioned, with information only being relayed verbally. Nevertheless, participants saw themselves as being better prepared and able to assist others when statewide compulsory screening was implemented without prior training.
Inner setting
In light of prior experiences like school closures, quarantines, and challenges associated with remote learning, the intervention was perceived as less disruptive compared with other measures and associated with the hope for some continuity ‘at least until the summer break’ (school stakeholder 5).
Both children and teachers reported the study-based screening to be only a side topic, if at all, in their interactions at school, although participating teachers recounted how sometimes children talked about their experiences or the reasons why their parents were against testing in class. In general, participants perceived screenings (both as part of the study and following the introduction of compulsory screening) as being highly accepted.
Outer setting
Participants stated that their support of the study-based screening represented an attempt to increase their own safety, which they felt had been neglected by elected authorities. The subsequent introduction of compulsory screening therefore was appreciated by most participants, although concerns were voiced that a stricter control of testing fidelity than currently in place might be required, as not everyone was eager to comply.
Implementation process
The study was advocated by school stakeholders and also relied on those stakeholders for successful implementation. This resulted in high level of stakeholder ownership, which was seen as particularly relevant for study buy-in across respondent groups. The broad buy-in was particularly important given a context marked by a highly emotionalised debate around COVID-19 control measures in schools.
Respondents generally appreciated the chosen implementation process. Although the information sheets, particularly the information sheet for children, and the communication by school stakeholders were appreciated, respondents expected study participation to further increase with additional events and opportunities for potential respondents to ask questions directly of the study team prior to making a decision about participation (this opportunity was only offered to the parents’ association and staff, though not all parents).
Discussion
This study outlined experiences implementing home-based RDTs for universal screening in a primary school setting. The screening was highly accepted and viewed as feasible among interviewed participants. Negative consequences (eg, more risk-taking behaviour) were not observed. However, concerns surfaced regarding the broad utility of screening when many individuals within a social setting may decline participation or not perform tests as advised. Interviewed participants expected screening acceptance and motivation to increase if the test was perceived to have consequences beyond a heightened sense of personal security. No case of SARS-CoV-2 was detected via the screening in the context of this study, and no clusters of infections indicated undetected cases.
Our findings regarding the screening’s feasibility mirror outcomes of projects that implemented self-sampling for SARS-CoV-2 testing in school settings.26 27 However, this evidence stems from secondary schools27 or from oral self-sampling.26 The high acceptance of screening expressed by our participants mirrors qualitative evidence regarding the acceptance of broader COVID-19 prevention measures in schools in the UK.10 We expand on this evidence by highlighting the acceptability and feasibility of home-based nasal sampling among primary school pupils.
The topic of large-scale RDT-based screening efforts in schools is emotionally highly charged in Germany, including lawsuits and homeschooling by parents who are fundamentally against SARS-CoV-2 testing for their children.8 Our findings highlight that an emotionally charged intervention can be generally acceptable to a target population if stakeholder buy-in and ownership is achieved through repeated explanations and demonstrations of the intervention.
Our study demonstrates that testing was perceived as less burdensome to participants, including pupils, than more established measures, such as facial masks. Considering the exceptional burden faced by schoolchildren and parents in the pandemic,28 and in light of increasing evidence regarding the impact of school closures on health and education29 30 and that children are at lower risk of severe disease progression,5 6 our results provide evidence that RDT-based screening is an acceptable and feasible way to facilitate in-person teaching. To the best of our knowledge, no positive cases (neither true positive nor false positive) emerged in the course of our study; we acknowledge however that a positive case may shift experiences with and perceptions of the intervention. We thus encourage further implementation research that captures a true positive case (which could increase acceptability due to successfully avoiding potential transmission) or a false positive case (which could decrease acceptability due to concerns about test reliability).
Beyond COVID-19, one other public health measure relying on self-testing in school settings in high-income countries entails screening for head lice. A study in primary schools in Australia aimed to assess the reliability of home-based screening for head lice, and only found a sensitivity of parental reports of 16%.31 This suggests challenges when shifting testing from schools into the private realms, particularly in cases where a positive test result could be perceived as stigmatising or as having consequences for short-term school access. While this concern was also voiced by participating parents and educators in our study, the participation of over 50% of staff and parents probably reflects important distinctions between routine lice screening and self-testing amid a viral pandemic.
This study provides timely and in-depth qualitative data, producing insights into the real-life discourse amid rapidly changing regulations. The study site is representative for schools in periurban settings; research to date on health interventions at schools has predominantly focused on the urban context. However, our study also has limitations. First, only parents and pupils who had decided to voluntarily participate in the overarching screening programme could be recruited for interviews; critical voices therefore might be under-represented in the data on parents and their children. Additionally, we designed the screening approach in this study as a realistic scenario for large-scale rollout, which included PCR-based confirmatory testing only in cases where a positive RDT result was reported. To minimise screening-associated burden and to bolster participation, the research team together with school stakeholders also decided against asking participants to systematically report negative test results or the emergence of COVID-19-associated symptoms. No cluster of cases emerged in the study setting, suggesting that the screening did not systematically miss infections, but the biased collection of test result data inhibits broad statements regarding screening accuracy. Finally, as RDTs for SARS-CoV-2 have been introduced in Germany on a large scale in recent months, generalisability of our results to other countries where RDTs were less present in the public discourse might be limited.
RDT-based screening is an acceptable and easily scalable intervention to decrease risk of transmissions at schools and facilitate face-to-face teaching amid a pandemic. Policymakers should ensure comprehensive capacity building for testing, fit-for-purpose training materials for all age levels, and train-the-trainer programmes to enable scale up of universal screening. Furthermore, consistent communication on regulations and readily available support networks (hotlines via phone or email) can reduce burden for school staff and families.
Data availability statement
Considering the high public interest in research on COVID-19, qualitative data of participants who have indicated their agreement to this as part of the informed consent procedure can be shared with other researchers. However, to preserve the anonymity of respondents and considering the personal nature of qualitative data, requests will be considered on a case-by-case basis. Please contact the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The ethical review board at the Medical Faculty, Heidelberg University, Germany approved this study (S-141/2021).
Acknowledgments
We are grateful to all participants for their time and contribution.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SAM and CMD are joint senior authors.
Contributors NT and CMD conceived of the study. JW, NT, SAM and CMD conceptualised the study and data collection processes. JW, MS and NT implemented the study with support from SAM and CMD. JW collected and analysed the data, supported by all coauthors. JW drafted the manuscript. All coauthors contributed to data interpretation, edited the manuscript and approved of the final manuscript. CMD serves as a guarantor for this study.
Funding This study was supported by a grant of the Ministry of Science, Research and the Arts of Baden-Württemberg, Germany, as well as hospital internal funds (grant numbers: not applicable). RDTs were provided free of cost by the manufacturer (Roche Diagnostics).
Disclaimer Funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf. CMD reports grants from Ministry of Science, Research and the Arts of Baden-Württemberg, Germany, grants from Heidelberg University Hospital internal funds, non-financial support from Roche Diagnostics (grant numbers: not applicable) during the conduct of the study. NT reports her children receiving RDTs as part of their participation in the screening programme. JW, MS and SAM report no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.